
Appendectomy
An appendectomy is the surgical removal of the appendix, most often performed to treat acute appendicitis, a condition where the appendix becomes inflamed and infected. If untreated, it may rupture and cause serious infection in the abdomen.
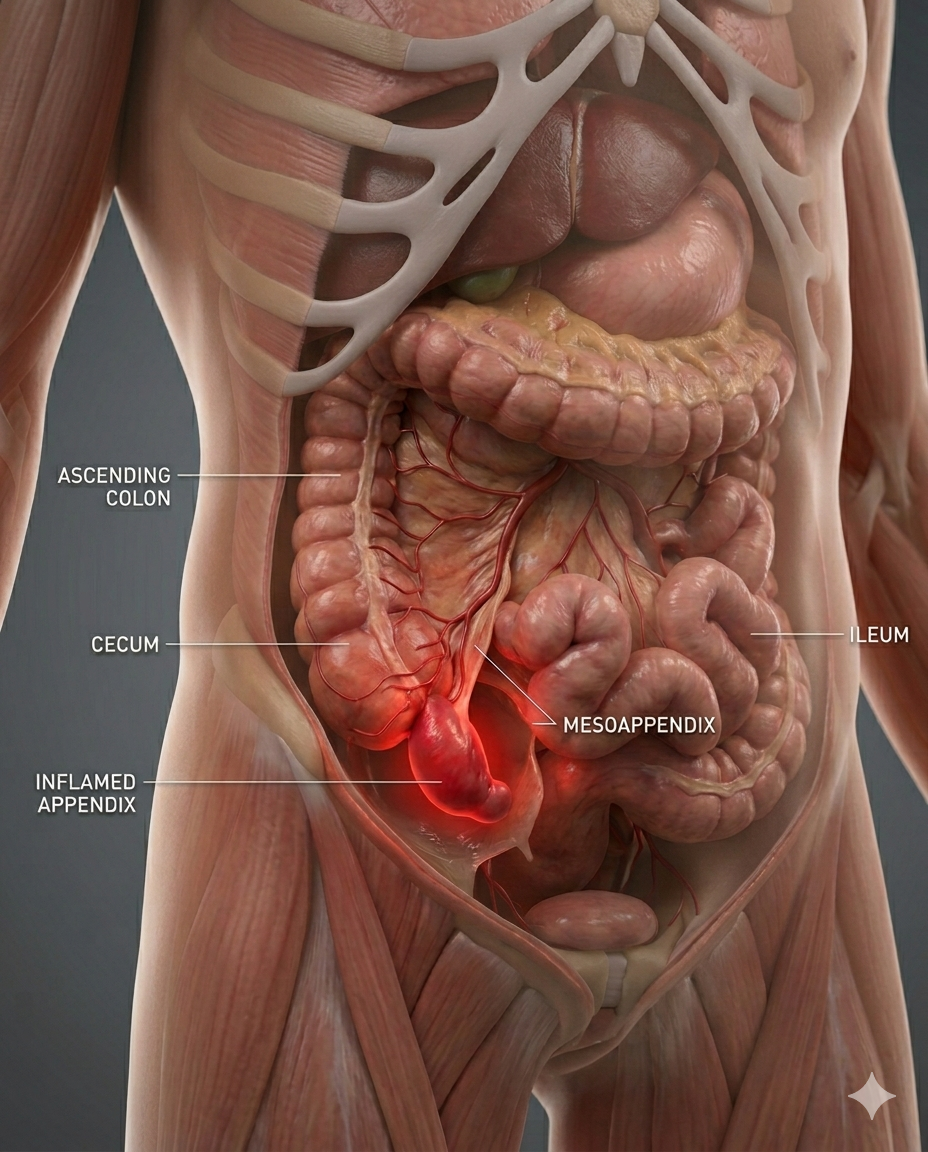
Medical illustration of Acute Appendicitis inside the human abdomen, transparent torso view, realistic cecum and inflamed appendix glowing red, surrounding bowel anatomy visible.
Appendectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains appendicitis, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
An Appendectomy is a surgical procedure performed to remove the appendix, a small, tube-shaped organ attached to the beginning of the large intestine (cecum) in the lower right abdomen.
This procedure is most commonly performed to treat appendicitis, a condition where the appendix becomes inflamed, swollen, or infected. If untreated, the appendix can rupture (perforate), leading to serious complications such as infection throughout the abdomen (peritonitis) or abscess formation.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Appendectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-facing version:
Patient-facing:
An appendectomy is surgery to remove the appendix, usually because it is infected or inflamed. This condition is called appendicitis. If untreated, the appendix can rupture and cause infection inside the abdomen.Professional-facing:
Appendectomy is the operative removal of the vermiform appendix, most commonly for acute appendicitis. Approaches include laparoscopic, open, and robotic-assisted appendectomy, with laparoscopic being the dominant standard in many settings. -
Patient-Facing Version
Key structures:
Appendix
Cecum
Terminal ileum
Right lower quadrant
Mesoappendix
Appendiceal artery
Peritoneal cavity
Visual idea:
Interactive 3D abdomen showing the appendix attached to the cecum, with inflammation progression from early appendicitis to perforation. -
Appendectomy may be needed for:
Acute appendicitis
Perforated appendicitis
Appendiceal abscess
Gangrenous appendix
Recurrent/chronic appendicitis
• • Incidental appendix lesion or tumor
-
Typical evaluation includes:
History and physical exam
Right lower quadrant tenderness assessment
CBC / WBC count
CRP when used
CT abdomen/pelvis
Ultrasound, especially pediatric/pregnancy cases
Pregnancy test when appropriate
IV fluids
Antibiotics
NPO status
• • Surgical consent
-
Approach
Patient Explanation
Professional Notes
Laparoscopic
Small incisions, camera-guided removal
Standard minimally invasive approach
Open
Larger incision in right lower abdomen
Used for rupture, severe infection, difficult anatomy
Robotic
Surgeon controls robotic instruments
Less common, may help in complex anatomy or obese patients
Nonoperative antibiotics
Antibiotics without immediate surgery
Select uncomplicated cases only
-
Patient arrives and is evaluated
Imaging/labs confirm appendicitis
Antibiotics and fluids are started
Patient goes to OR
General anesthesia begins
Small ports are placed
Appendix is identified
Mesoappendix and blood supply are controlled
Appendix base is stapled, clipped, or tied
Appendix is removed in a specimen bag
Abdomen is inspected and irrigated if needed
Ports are closed
Patient recovers in PACU
Discharge same day or admission depending on severity
-
For appendectomy, the safety focus is clear identification before division.
Key safety checkpoints:
Confirm appendix origin from cecum
Identify appendiceal base
Control appendiceal artery
Avoid injury to cecum or terminal ileum
Assess for perforation or abscess
Remove appendix completely
Irrigate contaminated field when needed
LDS visual:
“Safe Appendectomy View” showing appendix, cecum, mesoappendix, artery, and staple/clamp zone. -
Common supplies:
Laparoscopic tower
5 mm / 10 mm camera
Trocars
Graspers
Maryland dissector
Energy device
Laparoscopic scissors
Endoscopic stapler
Endoloop or clips
Suction irrigator
Specimen retrieval bag
Suture closure kit
Industry categories:
Access devices
Visualization
Energy
Stapling
Specimen containment
Irrigation/suction
Closure products
-
Common medication categories:
Pre-op antibiotics
IV fluids
General anesthesia agents
Antiemetics
Pain control medications
Local anesthetic
Post-op oral analgesics
Antibiotics for perforated cases
-
Patient-facing risks:
Bleeding
Infection
Abscess
Bowel injury
Staple-line leak
Conversion to open surgery
Longer hospital stay if appendix ruptured
Anesthesia risks
Professional-facing complications:
Intra-abdominal abscess
Cecal injury
Ileus
Wound infection
Stump appendicitis
Port-site hernia
• • Sepsis in perforated disease
-
Typical recovery:
Same day: PACU recovery, walking, liquids
24–48 hours: Soreness, light diet, home care
3–7 days: Return to light activity
1–2 weeks: Many return to school/work
2–4 weeks: Full activity depending on case
• • Longer: Perforated appendicitis may require admission, drains, or antibiotics
-
Patient questions:
Is my appendix ruptured?
Can this be treated with antibiotics?
Am I a laparoscopic candidate?
How long will I stay in the hospital?
What are the warning signs after surgery?
When can I return to work or sports?
Will I need antibiotics after surgery?
LDS decision engine:
Diagnosis → Severity → Approach → Hospital capability → Surgeon match → Recovery plan
-
For clinicians, reps, and hospitals:
Procedure volume tracking
Device utilization mapping
Stapler vs endoloop preference
Energy-device preference
Pediatric vs adult workflows
Perforated vs nonperforated case segmentation
OR time benchmarking
Conversion rate tracking
Supply cost comparison
• • Surgeon/hospital appendectomy profile
