
C-Section
A Cesarean Section (C-Section) is surgery used to deliver a baby through the mother’s abdomen and uterus when vaginal delivery is not possible or safest.
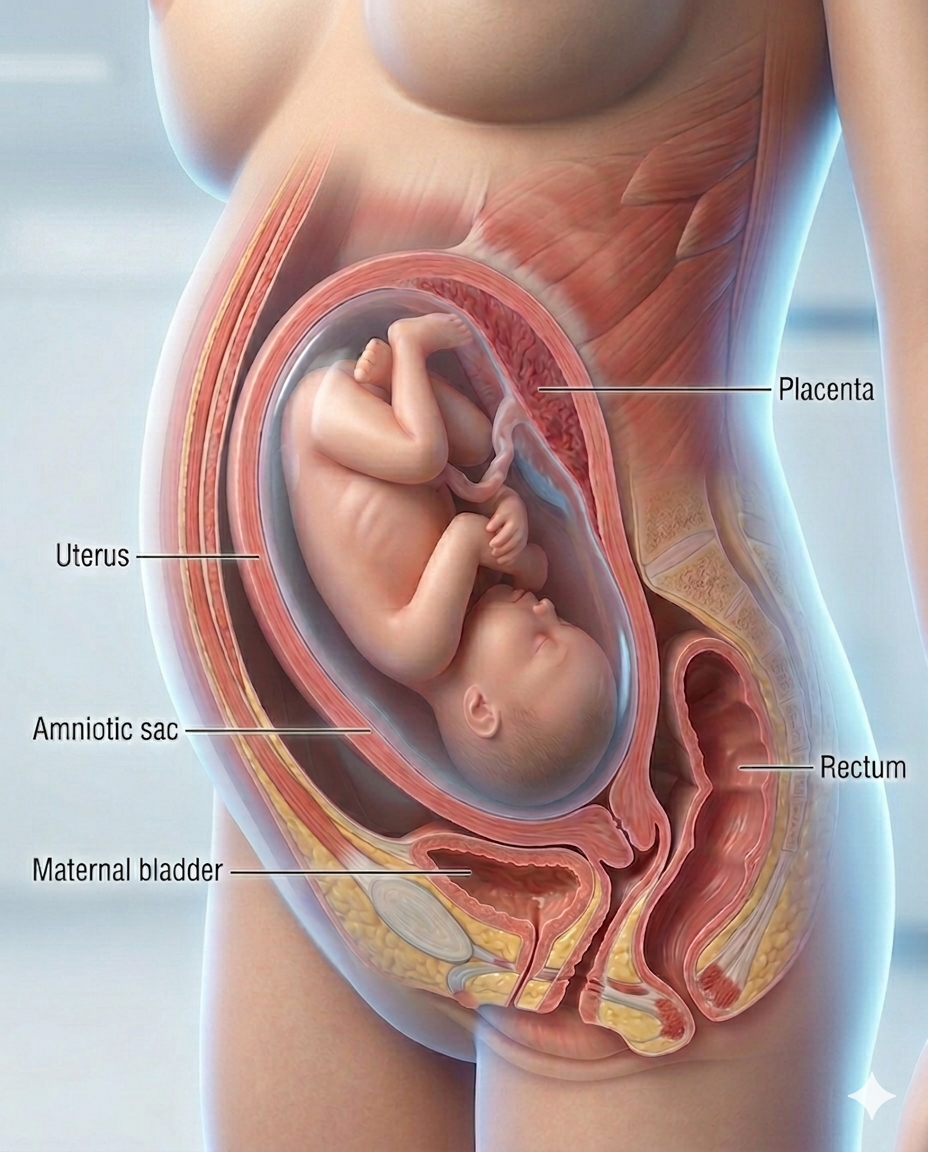
Medical illustration of a Full-Term Pregnant uterus inside a transparent female torso.
Cholecystectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains gallbladder disease, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
A cholecystectomy is the surgical removal of the gallbladder, most commonly done laparoscopically for symptomatic gallstones, cholecystitis, or related biliary disease. Laparoscopic surgery is the usual approach, while open surgery may be needed in more difficult or converted cases. Safe identification of the cystic duct and cystic artery using the Critical View of Safety is a core principle in modern cholecystectomy.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Cholecystectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-facing version:
A C-section, or cesarean delivery, is surgery used to deliver a baby through an incision in the abdomen and uterus. It may be planned ahead of time or performed urgently if vaginal delivery becomes unsafe for the mother, baby, or both. Common reasons include prior C-section, labor not progressing, fetal distress, breech position, twins or multiples, placenta problems, or certain maternal medical conditions. (ACOG)Professional-facing version:
Cesarean delivery is fetal delivery via laparotomy and hysterotomy. Core indications include labor dystocia, nonreassuring fetal status, malpresentation, placenta previa/accreta spectrum concerns, prior uterine surgery, multiple gestation scenarios, cord prolapse, and maternal/fetal contraindications to labor. (Merck Manuals) -
Key anatomy:
Skin, subcutaneous tissue, fascia, rectus muscles, peritoneum, bladder reflection, lower uterine segment, amniotic sac, placenta, umbilical cord, fetus, uterine vessels, cervix, fallopian tubes, ovaries.LDS visual idea:
“Layer-by-layer C-section anatomy” showing the path from skin incision → abdominal wall → uterus → baby delivery. -
Why a C-section may be needed:
Failure to progress, fetal distress, breech/transverse lie, placenta previa, placental abruption, prior C-section, uterine scar risk, multiple pregnancy, macrosomia concerns, cord prolapse, maternal infection concerns, severe preeclampsia, or emergency maternal/fetal instability.Patient message:
“The goal is not simply surgery — the goal is the safest delivery route for mother and baby.” -
Patient-facing:
Before a planned C-section, the care team reviews pregnancy history, prior deliveries, ultrasound findings, placenta location, fetal position, labs, allergies, anesthesia plan, medications, and blood type.Professional-facing:
CBC, type and screen, placenta localization, fetal assessment, anesthesia evaluation, antibiotic prophylaxis, aspiration prevention strategy, VTE risk assessment, hemorrhage risk stratification, neonatal team readiness when indicated. -
Planned C-section
Scheduled before labor begins.
Unplanned / urgent C-section
Performed after labor begins when vaginal delivery becomes unsafe.
Emergency C-section
Performed rapidly for immediate maternal or fetal danger.
Repeat C-section
Performed in patients with prior cesarean delivery.
VBAC / TOLAC alternative
Some patients with a prior low-transverse uterine incision may be candidates for trial of labor after cesarean; uterine rupture risk is low overall but clinically serious. (ACOG)
-
Patient arrives and is prepared
IV access, monitoring, fetal assessment
Spinal, epidural, or general anesthesia
Abdomen prepped and draped
Skin incision, usually low transverse
Abdominal wall opened layer by layer
Bladder protected
Uterine incision made
Baby delivered
Cord clamped and placenta delivered
Uterus repaired
Abdominal layers closed
Recovery room monitoring
• 14. Postpartum bonding, feeding, pain control, mobility
-
C-section “Critical View of Safety” equivalent:
Confirm correct patient, gestational status, fetal position, placenta location, bladder position, uterine incision site, hemorrhage readiness, antibiotic timing, neonatal readiness, and anesthesia stability.Key danger zones:
Bladder, uterine vessels, placenta, bowel adhesions in repeat surgery, lower uterine segment, fetal presenting part. -
Core supplies:
Scalpel, electrosurgery pencil, suction, retractors, laparotomy sponges, hemostats, forceps, needle drivers, Mayo/Metzenbaum scissors, bladder blade, uterine clamps, suture, skin closure system.OB-specific supplies:
Fetal delivery instruments, cord clamps, bulb suction, neonatal warmer, uterotonic medications, hemorrhage cart access, blood products when needed.Industry layer:
Closure devices, hemostatic agents, negative-pressure wound therapy, surgical drapes, fetal monitoring, anesthesia supplies, sutures, staplers, electrosurgery, suction/irrigation, OR integration. -
Common medication categories:
Antibiotic prophylaxis, spinal/epidural anesthetics, antiemetics, aspiration prophylaxis, uterotonics such as oxytocin, multimodal pain control, NSAIDs/acetaminophen when appropriate, opioids if needed, VTE prophylaxis for selected patients.Enhanced recovery angle:
Modern cesarean recovery pathways emphasize early feeding, early mobilization, multimodal analgesia, breastfeeding support, nausea control, and reducing unnecessary delays in recovery. (Ovid) -
Maternal risks:
Bleeding, infection, blood clots, anesthesia complications, injury to bladder/bowel/uterine vessels, wound problems, adhesions, longer recovery, and increased risks in future pregnancies including placenta problems, uterine rupture, and hysterectomy. (ACOG)Baby-related risks:
Breathing transition issues, accidental surgical injury, NICU evaluation when clinically needed.Future pregnancy risks:
Placenta previa, placenta accreta spectrum, uterine scar complications, repeat surgery complexity. -
Typical pathway:
Hospital stay often 2–4 days depending on hospital policy and patient condition. Early walking is encouraged. Pain, fatigue, incision soreness, bleeding, and emotional shifts are common. Full recovery often takes about 6 weeks, though this varies by patient. Mayo Clinic emphasizes incision care, pain control, activity limits, and warning signs during recovery. (Mayo Clinic)Warning signs:
Fever, worsening pain, heavy bleeding, foul-smelling discharge, incision redness/drainage, chest pain, shortness of breath, leg swelling, severe headache, vision changes, or mood crisis. -
Questions patients should ask:
Why is a C-section recommended for me?
Is this planned, urgent, or emergency?
What type of uterine incision is expected?
What anesthesia will I receive?
Can my support person be present?
What happens immediately after delivery?
What pain plan will I have?
What are my risks in future pregnancies?
Am I a VBAC candidate in the future?
• 10. What recovery signs should trigger a call?
-
Clinical dashboard fields:
Indication, urgency level, gestational age, fetal position, placenta location, prior uterine surgery, hemorrhage risk, anesthesia type, antibiotic timing, VTE risk, closure method, blood loss, neonatal status, complications, recovery pathway.Device/rep intelligence:
Closure systems, hemostatic products, wound therapy, sutures, electrosurgery, OR table/accessory setup, fetal monitoring, anesthesia supplies, neonatal equipment.LDS positioning:
C-section becomes a high-value module connecting patient education, OB workflow, supply intelligence, pharma mapping, recovery navigation, and maternal safety.Tagline:
“C-Section Intelligence: Safer Delivery Through Clearer Understanding.”
