
CABG
CABG stands for Coronary Artery Bypass Grafting. It is a type of open-heart surgery used to improve blood flow to the heart when the coronary arteries are blocked or severely narrowed.
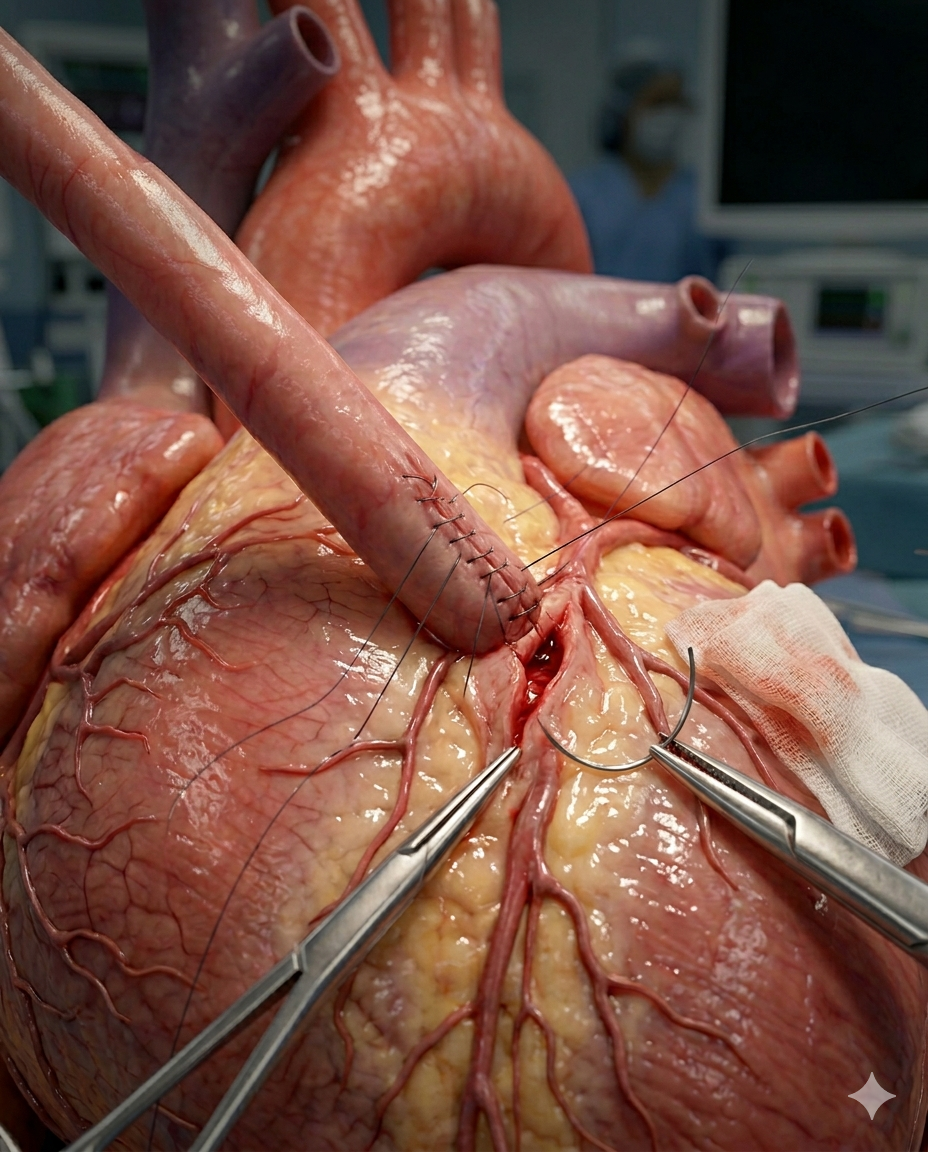
Left Internal Mammary Artery Bypass Graft to LAD Coronary Artery, close-up cardiothoracic surgery anatomy, delicate vascular suturing, coronary circulation restored.
Cholecystectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains gallbladder disease, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
A cholecystectomy is the surgical removal of the gallbladder, most commonly done laparoscopically for symptomatic gallstones, cholecystitis, or related biliary disease. Laparoscopic surgery is the usual approach, while open surgery may be needed in more difficult or converted cases. Safe identification of the cystic duct and cystic artery using the Critical View of Safety is a core principle in modern cholecystectomy.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Cholecystectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
CABG means Coronary Artery Bypass Grafting. It treats blocked coronary arteries by using a healthy blood vessel from the chest, arm, or leg to create a new route for blood to reach the heart muscle. (www.heart.org)
Patient-facing:
CABG is heart bypass surgery. Instead of opening the blockage directly, the surgeon builds a “detour” around it so oxygen-rich blood can reach the heart again.Professional-facing:
CABG is surgical myocardial revascularization for obstructive coronary artery disease, commonly using LIMA/internal thoracic artery, radial artery, and/or saphenous vein conduits. -
Key anatomy:
Heart muscle — the pump that needs oxygenated blood.
Coronary arteries — LAD, RCA, circumflex, diagonal, obtuse marginal, PDA branches.
Aorta — source vessel for many bypass grafts.
Internal mammary/internal thoracic artery — common arterial graft, especially to LAD.
Saphenous vein — common leg vein conduit.
Radial artery — arm artery conduit option.LDS visual:
“Blocked coronary artery → graft detour → restored blood flow.” -
CABG is usually considered for:
Coronary artery disease
Left main disease
Multivessel CAD
Diabetic multivessel CAD
Failed or unsuitable PCI/stenting
Ongoing angina despite medication
Reduced heart function with surgically treatable blockagesCABG can improve blood flow, reduce angina, improve exercise tolerance, and may improve survival in selected high-risk anatomy. (Mayo Clinic)
-
Typical pre-op intelligence layer:
Cardiac testing: coronary angiogram, echocardiogram, EKG, stress testing when appropriate.
Risk assessment: EF, diabetes, kidney disease, lung disease, prior stroke, frailty, anticoagulation, prior sternotomy.
Conduit planning: vein mapping, radial artery assessment, internal mammary artery suitability.
Medication review: antiplatelets, anticoagulants, beta blockers, statins, diabetes meds.
Patient prep: anesthesia evaluation, bloodwork, chest imaging, infection prevention, education. -
1. Traditional on-pump CABG
Median sternotomy, cardiopulmonary bypass, arrested heart.2. Off-pump CABG
Beating-heart bypass without heart-lung machine in selected cases.3. Minimally invasive CABG / MIDCAB
Smaller incision, often focused on LAD/LIMA grafting.4. Robotic-assisted CABG / hybrid coronary revascularization
Selected patients; may combine robotic LIMA harvest or minimally invasive bypass with PCI. -
Anesthesia and monitoring
Sternotomy or minimally invasive access
Conduit harvest: internal mammary, radial, saphenous vein
Heparinization
Cardiopulmonary bypass setup if on-pump
Heart stabilization or arrest
Distal coronary targets identified
Graft sewn below blockage
Proximal graft attached to aorta if needed
Flow confirmed
Weaning from bypass if used
Hemostasis
Chest tubes and pacing wires placed
Sternum/chest closed
• 15. ICU recovery
-
For CABG, the “critical safety view” is not Calot’s Triangle — it is myocardial protection + graft strategy + target verification.
Critical CABG safety checkpoints:
Correct patient / correct vessels / correct targets
Confirmed coronary anatomy from angiogram
Adequate conduit quality
Safe cannulation and cross-clamp strategy
Myocardial protection plan
Graft orientation without twist or tension
Anastomosis quality
Graft flow verification
Bleeding control before closure -
Capital equipment:
Heart-lung machine, heater-cooler, cell saver, anesthesia monitor, TEE, electrocautery, sternal saw.Core surgical supplies:
Sternal wires/plates, vascular clamps, coronary shunts, vessel loops, pledgets, fine sutures, clips, chest tubes, pacing wires.Conduit tools:
Endoscopic vein harvest system, radial harvest set, internal mammary retractors.Monitoring:
TEE probe, arterial line, central line, Swan-Ganz catheter when used.Procedure Builder logic:
Approach → conduit choice → target vessels → bypass count → pump strategy → closure system → ICU pathway. -
Pre-op / peri-op:
Antibiotic prophylaxis, beta blocker when appropriate, statin therapy, anticoagulation plan.Intra-op:
Heparin, protamine reversal, vasoactive medications, cardioplegia solution, antiarrhythmics as needed.Post-op:
Aspirin, statin, beta blocker, blood pressure control, diabetes control, pain management, DVT prophylaxis, possible dual antiplatelet therapy depending on patient factors.Long-term outcomes depend heavily on controlling blood pressure, cholesterol, diabetes, and medication adherence. (Mayo Clinic)
-
Key risks:
Bleeding
Infection
Stroke
Heart attack
Arrhythmias, especially atrial fibrillation
Kidney injury
Respiratory complications
Graft failure
Wound complications
Cognitive changes
DeathPatient-specific risk changes significantly based on age, EF, diabetes, kidney disease, lung disease, urgency, and overall frailty.
-
Typical recovery:
ICU: first 1–2 days depending on stability.
Hospital stay: often several days.
Home recovery: fatigue, incision care, walking program, breathing exercises.
Full recovery: commonly 6–12 weeks after discharge for traditional CABG; minimally invasive CABG may recover faster. (NHLBI, NIH)
Cardiac rehab: major recovery accelerator. -
Questions patients should ask:
Why do I need bypass instead of stents or medicine?
How many vessels need bypass?
Which grafts will be used?
Will this be on-pump or off-pump?
What is my personal risk score?
How long will I be in ICU?
What does recovery look like at 2, 6, and 12 weeks?
Will I need cardiac rehab?
How do I prevent future blockages?LDS patient promise:
“Understand your heart, your blockages, your bypass plan, and your recovery before you enter the OR.” -
CABG Builder Fields
Patient factors: EF, diabetes, renal function, COPD, prior PCI, prior sternotomy, frailty.
Anatomy: left main, LAD, RCA, circumflex, OM, diagonal, PDA targets.
Approach: on-pump, off-pump, MIDCAB, robotic-assisted, hybrid.
Conduits: LIMA, RIMA, radial, SVG.
Bypass count: single, double, triple, quadruple+.
Technology: TEE, epiaortic ultrasound, graft flow measurement, endoscopic harvest.
ICU pathway: extubation plan, pressors, rhythm monitoring, chest tube management.
Post-op pathway: antiplatelet, statin, rhythm control, wound care, rehab.Monetizable LDS overlays:
Device stack, conduit harvest tools, closure systems, ICU monitoring, cardiac rehab referral, pharma adherence pathway, surgeon/hospital CABG volume, robotic/minimally invasive availability.
