
A cholecystectomy is surgery to remove the gallbladder.
The gallbladder is a small pouch located underneath the liver. Its job is to store bile, a digestive fluid made by the liver that helps break down fats.
When gallstones block the normal flow of bile, the gallbladder can become painful, swollen, infected, or dangerous. Removing the gallbladder can relieve symptoms and help prevent serious complications.
Cholecystectomy
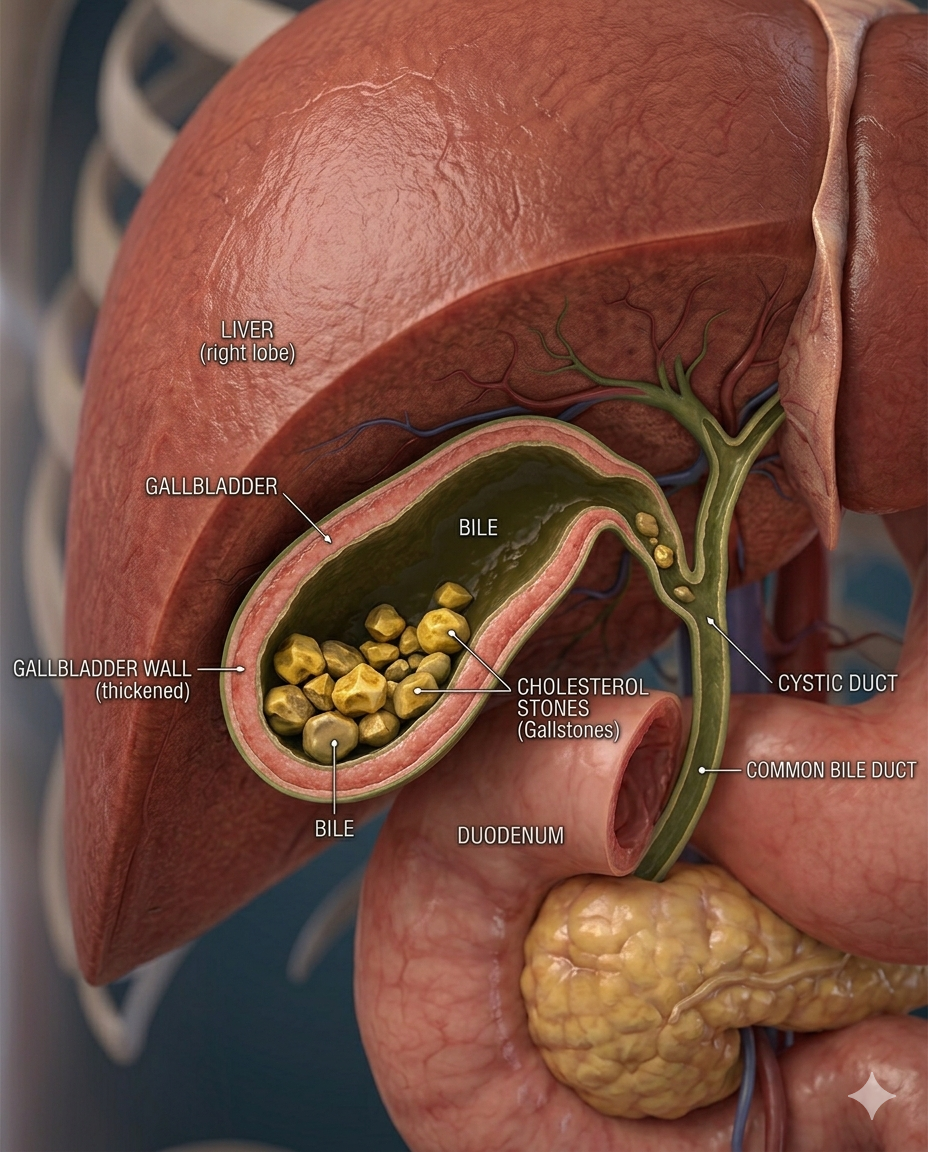
Medical illustration of a Gallbladder with Cholelithiasis, showing multiple yellow cholesterol stones inside the gallbladder lumen, mildly thickened gallbladder wall, bile fluid, and surrounding Liver anatomy. Patient-friendly cross-section.
Cholecystectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains gallbladder disease, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
A cholecystectomy is the surgical removal of the gallbladder, most commonly done laparoscopically for symptomatic gallstones, cholecystitis, or related biliary disease. Laparoscopic surgery is the usual approach, while open surgery may be needed in more difficult or converted cases. Safe identification of the cystic duct and cystic artery using the Critical View of Safety is a core principle in modern cholecystectomy.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Cholecystectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-facing version
A cholecystectomy is surgery to remove the gallbladder.
The gallbladder is a small pouch under the liver that stores bile. Bile helps digest fat. When gallstones, inflammation, infection, or blockage occur, the gallbladder can cause pain, nausea, vomiting, fever, and serious complications.
Most gallbladder surgery is done using small incisions with a camera, called laparoscopic surgery. Some patients may be candidates for robotic cholecystectomy, which uses advanced 3D visualization and wristed instruments.
Professional-facing version
Cholecystectomy is the surgical removal of the gallbladder, most commonly performed for symptomatic cholelithiasis, acute or chronic cholecystitis, biliary dyskinesia, gallstone pancreatitis after stabilization, or gallbladder polyps with concerning features.
Primary approaches include:
Laparoscopic cholecystectomy
Robotic-assisted cholecystectomy
Open cholecystectomy
Subtotal or fenestrating cholecystectomy in hostile anatomy
Core safety objective: obtain the Critical View of Safety before clipping/dividing ductal or vascular structures.
-
Key structures
Gallbladder
Stores bile produced by the liver.
Liver
Produces bile and sits directly above the gallbladder.
Cystic duct
Connects the gallbladder to the common bile duct.
Common bile duct
Carries bile from the liver and gallbladder area into the small intestine.
Cystic artery
Blood supply to the gallbladder.
Calot’s Triangle
Important surgical zone bordered by:
Cystic duct
Common hepatic duct
Inferior edge of the liver
This is where surgeons identify the cystic duct and cystic artery.
-
Common reasons for surgery
Symptomatic gallstones
Gallstones cause recurring right upper abdominal pain, often after fatty meals.
Acute cholecystitis
Inflamed or infected gallbladder, often requiring urgent surgery.
Chronic cholecystitis
Long-term irritation from gallstones.
Biliary dyskinesia
Poor gallbladder emptying despite no stones.
Gallstone pancreatitis
Gallstones block bile/pancreatic drainage and inflame the pancreas.
Gallbladder polyps
Some polyps require removal depending on size and risk profile.
-
Patient-facing
Before surgery, patients may need:
Physical exam
Blood work
Liver function tests
Ultrasound
CT scan or HIDA scan in selected cases
Review of medications
Anesthesia evaluation
Professional-facing
Typical evaluation includes:
CBC
CMP
LFTs
Bilirubin
Lipase if pancreatitis suspected
RUQ ultrasound
HIDA scan for dyskinesia or equivocal cholecystitis
MRCP/ERCP consideration if choledocholithiasis suspected
Antibiotics for acute infection when indicated
• • DVT prophylaxis based on risk
-
Laparoscopic cholecystectomy
Most common approach. Uses small incisions, camera, laparoscopic instruments, clips, and electrosurgery.
Robotic cholecystectomy
Uses robotic arms, 3D visualization, wristed instruments, and may include Firefly fluorescence imaging with ICG to help visualize biliary anatomy.
Open cholecystectomy
Larger incision. Used when anatomy is unsafe, inflammation is severe, bleeding occurs, or conversion is needed.
Subtotal cholecystectomy
Used when full removal is unsafe due to severe inflammation or distorted anatomy.
-
Patient version
You receive anesthesia.
Small incisions are made.
The abdomen is inflated with CO₂ gas.
A camera is inserted.
The surgeon identifies the gallbladder.
The cystic duct and artery are carefully exposed.
Safety anatomy is confirmed.
The duct and artery are clipped and divided.
The gallbladder is removed from the liver bed.
It is placed in a bag and removed.
Incisions are closed.
You recover in the post-anesthesia area.
Professional version
Supine positioning
General anesthesia
Veress or Hasson entry
Pneumoperitoneum
Trocar placement
Diagnostic laparoscopy
Retraction of fundus and infundibulum
Dissection of hepatocystic triangle
Achieve Critical View of Safety
Clip/divide cystic duct
Clip/divide cystic artery
Gallbladder dissected off liver bed
Hemostasis and irrigation as needed
Specimen bag extraction
Port closure
• 16. PACU recovery
-
The Critical View of Safety is the key safety checkpoint in gallbladder surgery.
Before cutting anything, the surgeon should confirm:
Only two structures enter the gallbladder.
The lower third of the gallbladder is separated from the liver bed.
The hepatocystic triangle is cleared of fat and fibrous tissue.
LDS visual concept
Interactive 3D module showing:
Gallbladder
Cystic duct
Cystic artery
Common bile duct
Liver edge
Safe clip zone
Danger zone
• • Firefly/ICG toggle
-
Core equipment
Laparoscopic setup
Laparoscope
Camera system
Light source
Insufflator
Trocars
Graspers
Maryland dissector
Hook cautery
Clip applier
Suction irrigator
Specimen retrieval bag
Robotic setup
da Vinci Xi or da Vinci 5 platform
Robotic camera
Robotic trocars
Fenestrated bipolar forceps
Monopolar curved scissors
Cadiere forceps
Assistant port
Firefly fluorescence imaging
ICG dye
Clip and closure products
Titanium clips
Polymer locking clips
Endoscopic retrieval bag
Fascial closure device
• • Skin adhesive or sutures
-
Pre-op / intra-op medications
General anesthetics
Paralytics
Opioid or non-opioid analgesics
Antiemetics
Antibiotics when indicated
ICG for fluorescence imaging when used
Local anesthetic at port sites
Post-op medications
Acetaminophen
NSAIDs if appropriate
Limited opioid prescription if needed
Antiemetics
• • Stool softener if opioids are used
-
Patient-facing risks
Bleeding
Infection
Bile leak
Injury to the bile duct
Injury to nearby organs
Blood clots
Hernia at incision site
Need to convert to open surgery
Continued abdominal symptoms in some patients
Professional-facing complications
Common bile duct injury
Right hepatic duct injury
Cystic duct stump leak
Bile leak from liver bed or duct of Luschka
Vascular injury
Retained common bile duct stone
Post-op abscess
Port-site hernia
Conversion to open
• • Need for ERCP or reoperation
-
Typical recovery timeline
Same day
Many patients go home the same day.
First 24–48 hours
Soreness, bloating, shoulder discomfort from gas, mild nausea.
First week
Light walking encouraged. Avoid heavy lifting.
1–2 weeks
Many patients return to desk work or light activity.
2–4 weeks
Most patients return to normal activity depending on surgeon instructions.
Red flags
Patients should contact their care team for:
Fever
Worsening abdominal pain
Yellow skin or eyes
Persistent vomiting
Chest pain
Shortness of breath
Drainage or redness at incision sites
Dark urine or pale stools
-
LDS Decision Engine Questions
Do you have gallstones?
Are you having pain after meals?
Have you had fever, nausea, or vomiting?
Was your diagnosis acute or chronic?
Has your doctor recommended surgery?
Are you interested in laparoscopic vs robotic options?
Do you want to know which hospitals near you offer advanced imaging or robotic technology?
Do you want help preparing questions for your surgeon?
Suggested patient CTA
Understand your gallbladder surgery before you schedule it.
Compare laparoscopic, robotic, and open approaches. Learn what devices may be used, what recovery looks like, and what questions to ask your surgeon. -
Surgeon-facing data fields
Approach preference
Case volume
Robotic availability
Firefly/ICG usage
Clip preference
Energy device preference
Conversion rate
Bile duct injury prevention protocol
Acute cholecystitis management strategy
Subtotal cholecystectomy threshold
ERCP referral pathway
Hospital outpatient capability
Rep-facing opportunity layer
Device companies
Robotic platform placement
Fluorescence imaging adoption
Clip systems
Retrieval bags
Energy devices
Trocars
Visualization systems
Pharma companies
ICG
Antibiotics
Antiemetics
Non-opioid pain pathways
ERAS-related medications
LDS Positioning Statement
Cholecystectomy is not just gallbladder removal. It is a high-volume surgical pathway where patient education, surgeon decision-making, device selection, imaging technology, and recovery planning all intersect.
Let’s Do Surgery turns that pathway into a clear, visual, connected experience.
