
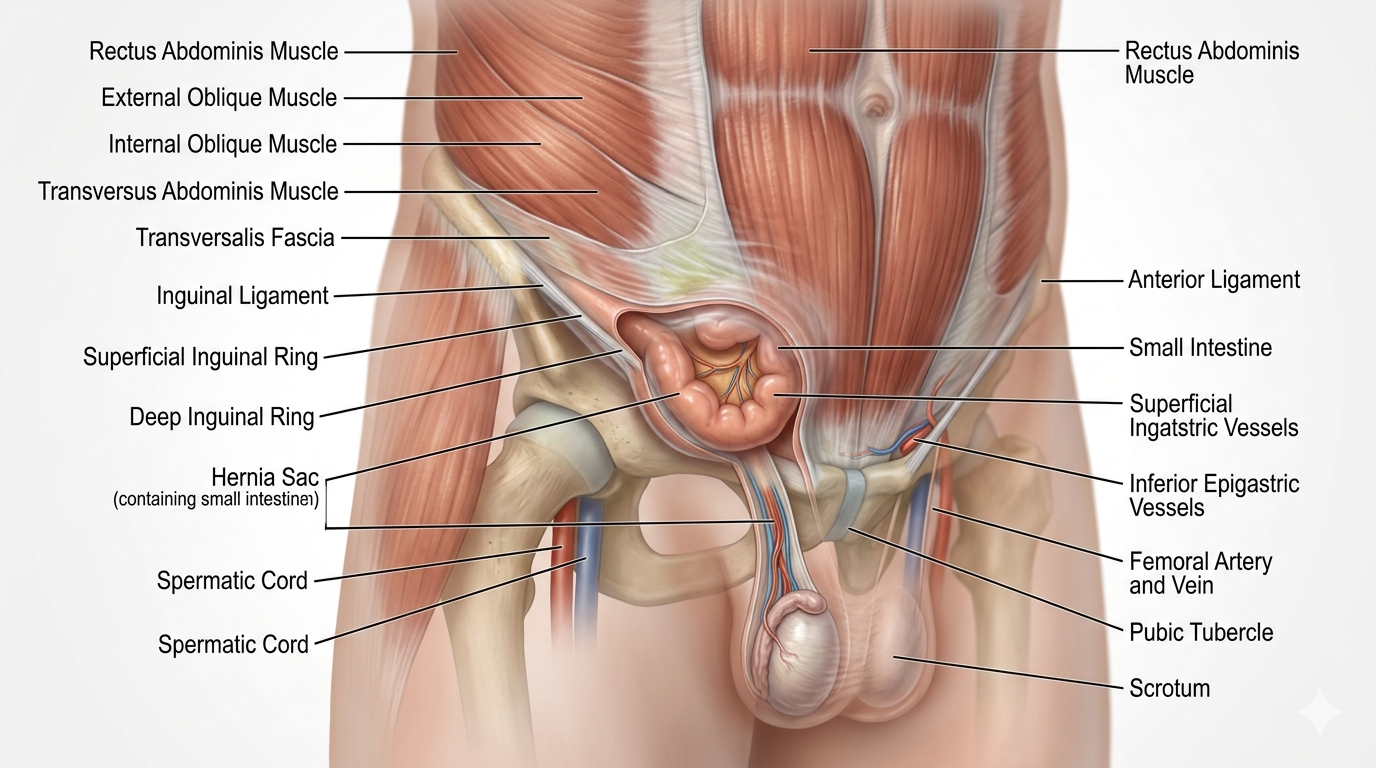
Hernia Repair is a surgical procedure used to fix a hernia, which occurs when an organ, fatty tissue, or part of the intestine pushes through a weak area or opening in the muscle or connective tissue (fascia).
The goal of hernia repair is to:
Return the protruding tissue to its normal position
Repair or strengthen the weakened abdominal wall or tissue
Reduce pain or discomfort
Prevent complications such as incarceration or strangulation
Hernia Repair
Medical illustration of a Gallbladder with Cholelithiasis, showing multiple yellow cholesterol stones inside the gallbladder lumen, mildly thickened gallbladder wall, bile fluid, and surrounding Liver anatomy. Patient-friendly cross-section.
Cholecystectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains gallbladder disease, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
A cholecystectomy is the surgical removal of the gallbladder, most commonly done laparoscopically for symptomatic gallstones, cholecystitis, or related biliary disease. Laparoscopic surgery is the usual approach, while open surgery may be needed in more difficult or converted cases. Safe identification of the cystic duct and cystic artery using the Critical View of Safety is a core principle in modern cholecystectomy.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Cholecystectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-facing version:
A hernia happens when tissue, fat, or intestine pushes through a weak spot in the muscle wall. Hernia repair closes that weak area, often with sutures and/or surgical mesh to reinforce the repair. Common types include inguinal, femoral, umbilical, ventral, incisional, hiatal, and parastomal hernias. Surgery may be open, laparoscopic, or robotic. ACS notes that surgery is the only definitive repair for many hernias, though watchful waiting may be appropriate for some reducible, minimally symptomatic hernias. (ACS)Professional-facing version:
Hernia repair restores abdominal wall integrity, reduces risk of incarceration/strangulation, relieves symptoms, and lowers recurrence risk through defect closure, mesh reinforcement, or both. Technique depends on hernia type, defect size, prior surgery, contamination risk, patient BMI/comorbidities, tissue quality, and recurrence status. -
Core anatomy:
Abdominal wall layers: skin, subcutaneous tissue, fascia, muscle, peritoneum.
Key hernia zones: inguinal canal, femoral canal, umbilicus, linea alba, prior incision sites, and parastomal defects.Visual LDS elements:
3D abdominal wall map, hernia bulge animation, mesh placement overlay, nerve/vessel danger-zone labels, recurrence-risk heat map. -
Common hernia categories:
Hernia Type
Location
Key Concern
Inguinal
Groin
Most common; direct or indirect
Femoral
Below inguinal ligament
Higher incarceration risk
Umbilical
Belly button
Common in adults with obesity/pregnancy history
Ventral
Abdominal wall
Primary abdominal wall weakness
Incisional
Prior surgical incision
Fascial failure after surgery
Hiatal
Diaphragm/stomach
Reflux/paraesophageal risk
Parastomal
Around ostomy
Complex recurrence risk
-
Patient-facing:
Evaluation includes physical exam, symptom review, hernia size, reducibility, pain, prior surgeries, and sometimes CT or ultrasound.Professional-facing:
Assess reducibility, defect size, loss of domain, bowel involvement, prior mesh, infection history, anticoagulation, smoking, diabetes, BMI, nutrition, and contamination risk. CT is especially useful for complex ventral/incisional/recurrent hernias. -
Approach
Best For
Advantages
Tradeoffs
Open repair
Large, complex, recurrent, contaminated cases
Direct access, flexible reconstruction
Larger incision, more wound morbidity
Laparoscopic repair
Selected ventral/inguinal cases
Smaller incisions, faster recovery
Requires intraperitoneal access, fixation considerations
Robotic repair
Ventral, inguinal, complex abdominal wall reconstruction
Enhanced suturing, 3D visualization, retromuscular options
Cost, setup time, platform availability
SAGES describes laparoscopic/robotic hernia repair as minimally invasive approaches using small incisions, specialized instruments, and often mesh, with many patients experiencing easier recovery and faster return to activity compared with open repair. (SAGES)
-
Core laparoscopic workflow:
1. Patient positioning
2. Anesthesia and prep
3. Port placement
4. Abdominal entry and insufflation
5. Retraction of gallbladder
6. Exposure of hepatocystic triangle
7. Dissection of peritoneum
8. Achieve Critical View of Safety
9. Clip and divide cystic duct
10. Clip and divide cystic artery
11. Separate gallbladder from liver bed
12. Hemostasis and irrigation
13. Retrieval bag extraction
14. Closure and dressing
SAGES recommends the Critical View of Safety for anatomic identification of the cystic duct and cystic artery during laparoscopic cholecystectomy as part of safe cholecystectomy practice.
-
This should be one of the strongest parts of LDS.
Teach the 3 components:
• Clear the hepatocystic triangle of fat and fibrous tissue
• Separate the lower third of the gallbladder from the cystic plate
• Confirm that only two structures enter the gallbladder
Digital tools:
• “CVS achieved / not achieved” visual quiz
• surgeon mode with operative image annotation
• AI overlay for duct and artery recognition
• safety timeout checkpoint before clipping
-
Break it down by category:
Access
• Veress needle or optical trocar
• 5 mm / 10–12 mm trocars
Visualization
• laparoscope
• camera head
• light source
• insufflator
Dissection
• Maryland dissector
• hook cautery
• blunt grasper
• atraumatic grasper
• suction irrigator
Hemostasis / division
• clip applier
• laparoscopic clips
• energy device if used
Specimen handling
• endoscopic retrieval bag
Closure
• fascial closure device
• sutures
• skin adhesive / steri-strips / staples
LDS feature:
Every step opens the relevant devices, manufacturers, SKU fields, rep contacts, and preference-card notes.
-
Include:
• general anesthetics
• peri-op antibiotics when indicated
• analgesics
• antiemetics
• local anesthetic at port sites
• VTE prophylaxis per protocol
• indocyanine green if fluorescence cholangiography is used
-
Patient-friendly and professional versions should both be included.
Commonly discussed risks include:
• bleeding
• infection
• bile leak
• bile duct injury
• retained stones
• injury to bowel or liver
• need to convert to open surgery
• DVT/PE
• anesthesia-related complications
NHS and hospital discharge materials also emphasize gradual recovery, mobility, and awareness of complications after surgery.
-
Most patients having laparoscopic gallbladder removal recover faster than those having open surgery and may return to work in roughly 1–2 weeks depending on job demands, while open surgery usually involves a longer recovery.
Recovery module should include:
• day of surgery
• pain expectations
• diet progression
• walking and mobility
• wound care
• lifting restrictions
• return-to-work timeline
• when to call the surgeon
• emergency red flags
-
Include:
• Why remove the gallbladder?
• What happens if I wait?
• Will I still digest food normally?
• What are the alternatives?
• What happens during surgery?
• How long until I feel normal?
-
For surgeons / hospitals / reps:
• case type
• complexity score
• anatomy variant alerts
• preferred device stack
• conversion triggers
• intraoperative bailout strategy
• documentation checklist
• rep notification logic
• cost-per-case dashboard
