
Spine Fusion (also called Spinal Fusion) is a surgical procedure used to permanently join two or more vertebrae (bones of the spine) so they heal into one solid bone.
The goal is to stabilize the spine, reduce painful motion, and protect nerves or the spinal cord.
Spine Fusion
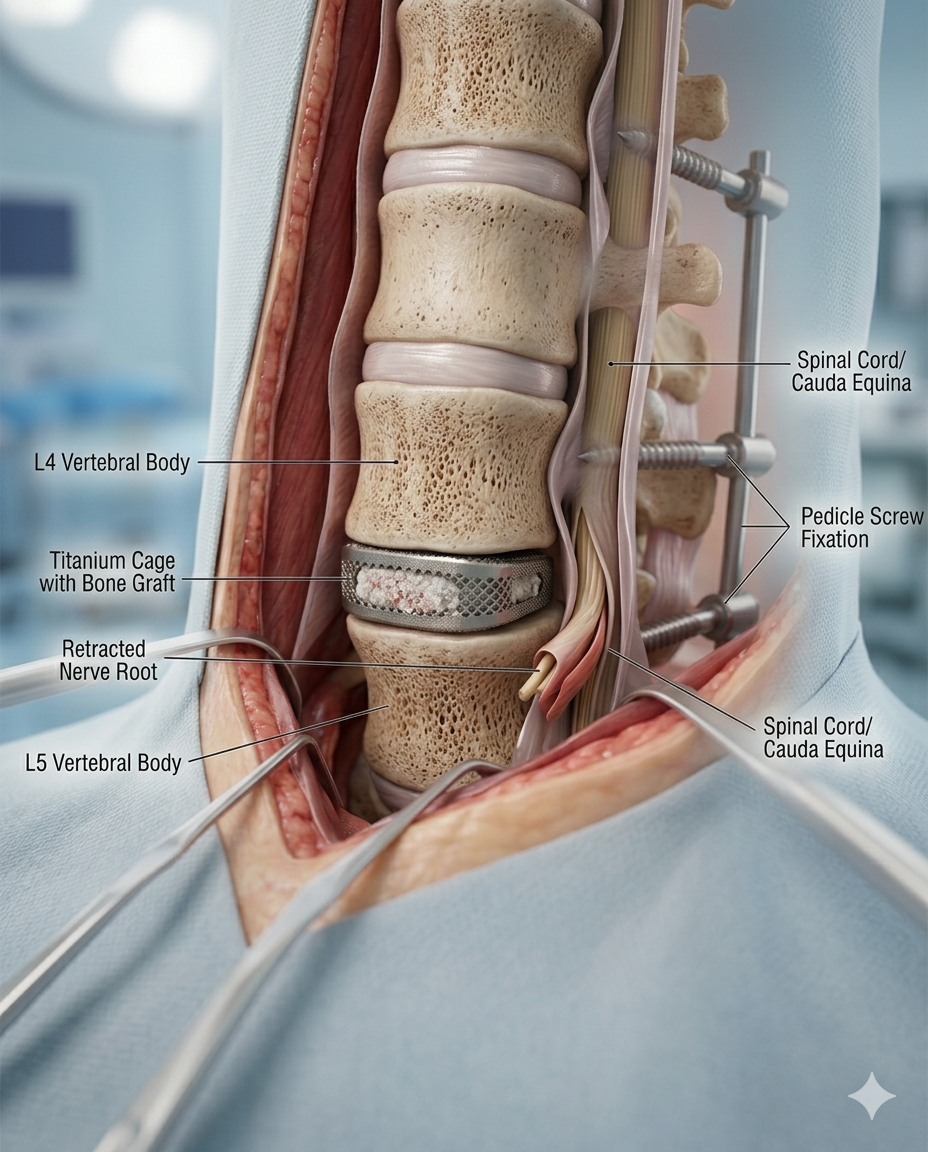
Titanium Fusion Cage positioned between vertebral bodies after disc removal, realistic bone graft material.
Cholecystectomy Digital Module
A guided, interactive, patient-to-professional digital experience that explains gallbladder disease, prepares the patient, maps the operation step by step, and connects anatomy, workflow, devices, risks, and recovery into one usable module.
A cholecystectomy is the surgical removal of the gallbladder, most commonly done laparoscopically for symptomatic gallstones, cholecystitis, or related biliary disease. Laparoscopic surgery is the usual approach, while open surgery may be needed in more difficult or converted cases. Safe identification of the cystic duct and cystic artery using the Critical View of Safety is a core principle in modern cholecystectomy.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Cholecystectomy: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-facing version:
Your gallbladder is a small organ under your liver that stores bile. If gallstones or inflammation cause pain, infection, or blockage, your doctor may recommend removing the gallbladder. Most people do well without it. Gallstones can cause pain and complications when they block bile ducts.
Professional-facing version:
Cholecystectomy is indicated for symptomatic cholelithiasis, acute or chronic cholecystitis, gallstone pancreatitis after stabilization, biliary dyskinesia in selected patients, and other gallbladder pathology. The standard operative approach is laparoscopic cholecystectomy, with selective conversion to open based on inflammation, adhesions, anatomy, bleeding, or concern for bile duct injury.
-
Include:
• Liver
• Gallbladder
• Cystic duct
• Common hepatic duct
• Common bile duct
• Cystic artery
• Right hepatic artery
• Calot’s triangle / hepatocystic triangle
• Cystic plate
• Duodenum
• Transverse colon
-
Include:
• Symptomatic gallstones
• Acute cholecystitis
• Chronic cholecystitis
• Choledocholithiasis
• Biliary colic
• Gallstone pancreatitis
• Gangrenous gallbladder
• Hydrops / empyema
-
Include:
• History and symptoms
• Physical exam
• CBC, CMP, LFTs
• Bilirubin
• Lipase if pancreatitis suspected
• Ultrasound as typical first-line imaging
• Possible MRCP / HIDA / CT depending on situation
• Anesthesia evaluation
• Antibiotic planning when indicated
NIDDK notes that clinicians may use blood tests and imaging such as ultrasound, CT, MRI, cholescintigraphy, or ERCP depending on the diagnostic question.
-
Include three pathways:
• Laparoscopic cholecystectomy
• Open cholecystectomy
• Robotic cholecystectomy
LDS logic:
Let the user toggle between approaches and compare:
• incision pattern
• visualization
• equipment
• recovery
• OR time
• training requirements
-
Core laparoscopic workflow:
1. Patient positioning
2. Anesthesia and prep
3. Port placement
4. Abdominal entry and insufflation
5. Retraction of gallbladder
6. Exposure of hepatocystic triangle
7. Dissection of peritoneum
8. Achieve Critical View of Safety
9. Clip and divide cystic duct
10. Clip and divide cystic artery
11. Separate gallbladder from liver bed
12. Hemostasis and irrigation
13. Retrieval bag extraction
14. Closure and dressing
SAGES recommends the Critical View of Safety for anatomic identification of the cystic duct and cystic artery during laparoscopic cholecystectomy as part of safe cholecystectomy practice.
-
This should be one of the strongest parts of LDS.
Teach the 3 components:
• Clear the hepatocystic triangle of fat and fibrous tissue
• Separate the lower third of the gallbladder from the cystic plate
• Confirm that only two structures enter the gallbladder
Digital tools:
• “CVS achieved / not achieved” visual quiz
• surgeon mode with operative image annotation
• AI overlay for duct and artery recognition
• safety timeout checkpoint before clipping
-
Break it down by category:
Access
• Veress needle or optical trocar
• 5 mm / 10–12 mm trocars
Visualization
• laparoscope
• camera head
• light source
• insufflator
Dissection
• Maryland dissector
• hook cautery
• blunt grasper
• atraumatic grasper
• suction irrigator
Hemostasis / division
• clip applier
• laparoscopic clips
• energy device if used
Specimen handling
• endoscopic retrieval bag
Closure
• fascial closure device
• sutures
• skin adhesive / steri-strips / staples
LDS feature:
Every step opens the relevant devices, manufacturers, SKU fields, rep contacts, and preference-card notes.
-
Include:
• general anesthetics
• peri-op antibiotics when indicated
• analgesics
• antiemetics
• local anesthetic at port sites
• VTE prophylaxis per protocol
• indocyanine green if fluorescence cholangiography is used
-
Patient-friendly and professional versions should both be included.
Commonly discussed risks include:
• bleeding
• infection
• bile leak
• bile duct injury
• retained stones
• injury to bowel or liver
• need to convert to open surgery
• DVT/PE
• anesthesia-related complications
NHS and hospital discharge materials also emphasize gradual recovery, mobility, and awareness of complications after surgery.
-
Most patients having laparoscopic gallbladder removal recover faster than those having open surgery and may return to work in roughly 1–2 weeks depending on job demands, while open surgery usually involves a longer recovery.
Recovery module should include:
• day of surgery
• pain expectations
• diet progression
• walking and mobility
• wound care
• lifting restrictions
• return-to-work timeline
• when to call the surgeon
• emergency red flags
-
Include:
• Why remove the gallbladder?
• What happens if I wait?
• Will I still digest food normally?
• What are the alternatives?
• What happens during surgery?
• How long until I feel normal?
-
For surgeons / hospitals / reps:
• case type
• complexity score
• anatomy variant alerts
• preferred device stack
• conversion triggers
• intraoperative bailout strategy
• documentation checklist
• rep notification logic
• cost-per-case dashboard
