
Total Knee Replacement
(Total Knee Arthroplasty, TKA)
Total Knee Replacement (TKR), also called Total Knee Arthroplasty (TKA), is a surgical procedure where a damaged or worn-out knee joint is replaced with artificial components designed to restore movement, stability, alignment, and pain relief.
Total Knee
Total Knee Anatomy:
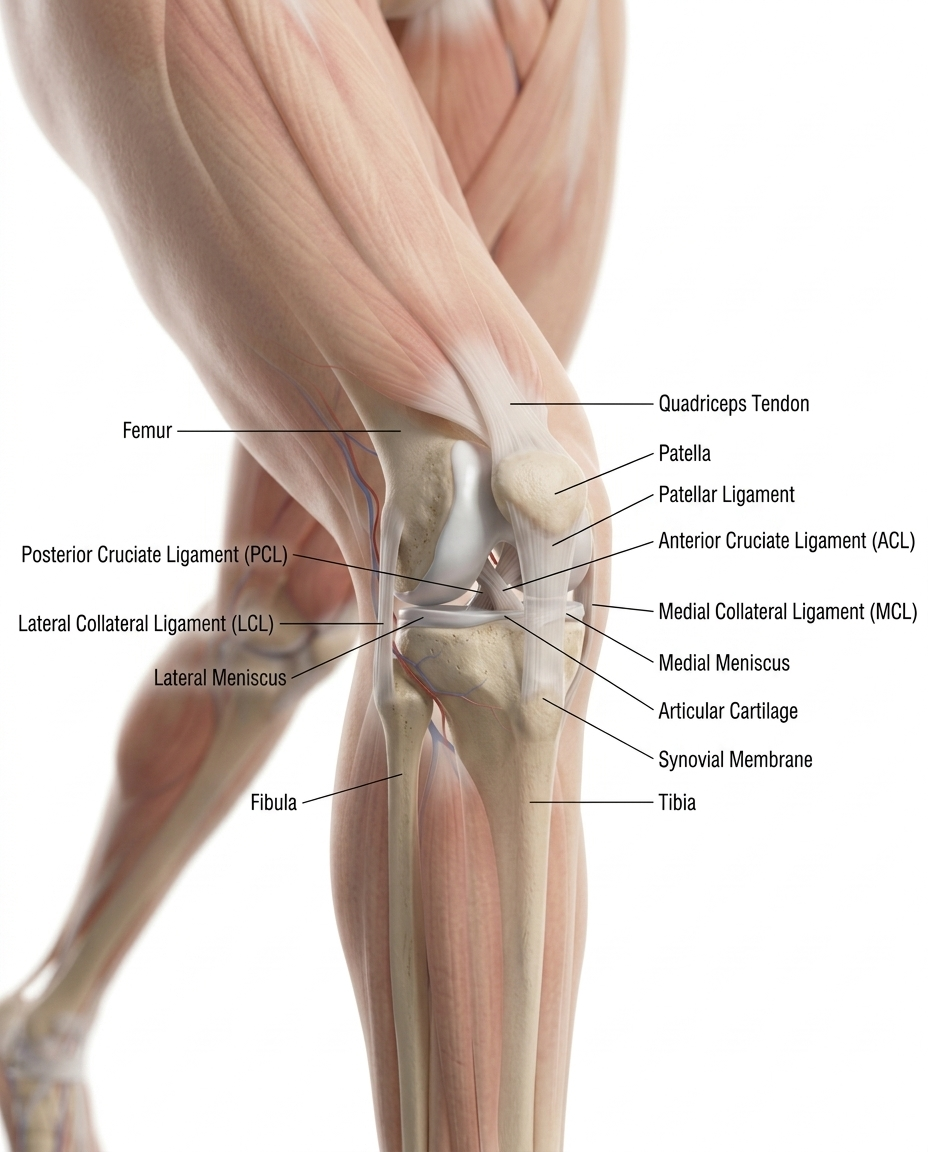
femur, tibia, fibula, patella, articular cartilage, meniscus, ACL, PCL, MCL, LCL, synovium, tendons and vascular anatomy..
Total Knee Digital Module
Patient-facing version:
A total knee replacement removes damaged cartilage and bone from the knee joint and replaces them with artificial components. The goal is to reduce pain, improve alignment, and help the patient return to walking and daily activity. AAOS describes total knee replacement as a safe and effective procedure when nonsurgical treatments no longer control arthritis symptoms. (OrthoInfo)
Professional-facing version:
Total knee arthroplasty replaces the diseased tibiofemoral and often patellofemoral joint surfaces with metal and polyethylene components. Indications commonly include end-stage osteoarthritis, inflammatory arthritis, post-traumatic arthritis, deformity, pain, and functional limitation despite conservative management.
-
This module should do four things at once:
1. Educate the patient in plain language
2. Support the surgeon and care team with structured workflow logic
3. Map devices, supplies, and pharma to each phase of the case
4. Create a reusable LDS digital product for web, app, LMS, and sales enablement.
-
A. Module title
Total Knee: A Guided Digital Surgical Experience
B. Module audience
• Patients and families
• Surgeons
• OR staff
• Hospitals
• Device reps
• Pharma partners
• Educators and training programs
-
Patient-Facing Version
Total Knee Replacement (Total Knee Arthroplasty – TKA)
What Is a Total Knee Replacement?
A Total Knee Replacement (TKA) is a surgical procedure used to replace a damaged or worn-out knee joint with artificial components called implants or prostheses.
The knee is one of the body’s largest and hardest-working joints. It helps you walk, bend, climb stairs, stand, and maintain balance. When the joint becomes damaged from arthritis, injury, or wear over time, movement can become painful and difficult.
A Total Knee Replacement removes damaged joint surfaces and replaces them with smooth artificial materials designed to:
Reduce pain
Restore movement
Improve stability
Help patients return to daily activities
Improve overall quality of life
⸻
Why Is Knee Replacement Done?
Total Knee Replacement is usually performed when knee pain and stiffness interfere with daily life and non-surgical treatments are no longer effective.
Common reasons include:
Osteoarthritis
The most common reason.
The protective cartilage in the knee wears away over time, causing:
Bone-on-bone contact
Pain
Swelling
Stiffness
Limited mobility
Rheumatoid Arthritis
An autoimmune disease that causes inflammation and damage inside the knee joint.
Post-Traumatic Arthritis
Arthritis that develops after:
Fractures
Ligament injuries
Meniscus damage
Previous knee trauma
Joint Deformity or Severe Instability
Some knees become:
Bowed inward or outward
Unstable
Difficult to support body weight
⸻
When Might Surgery Be Recommended?
Your surgeon may discuss Total Knee Replacement if you experience:
Chronic knee pain
Pain while walking or climbing stairs
Pain at rest or during sleep
Swelling that does not improve
Knee stiffness
Reduced mobility
Difficulty performing normal activities
Failure of non-surgical treatments
Non-surgical treatments often attempted first include:
Physical therapy
Weight management
Anti-inflammatory medications
Knee injections
Bracing
Activity modification
⸻
What Happens During Surgery?
During the procedure:
Step 1 — Anesthesia
You receive anesthesia so you are comfortable and pain-free.
This may include:
General anesthesia
Spinal anesthesia
Regional nerve blocks
⸻
Step 2 — Surgical Exposure
The surgeon makes an incision over the knee and carefully exposes the joint.
⸻
Step 3 — Removal of Damaged Surfaces
Damaged cartilage and small amounts of bone are removed from:
Femur (thigh bone)
Tibia (shin bone)
Sometimes the patella (kneecap)
⸻
Step 4 — Implant Placement
Artificial implants are positioned to recreate a smooth functioning joint.
Typical components include:
Femoral Component
Usually metal and attached to the thigh bone.Tibial Component
Metal base attached to the shin bone.Polyethylene Insert
Smooth plastic spacer that allows motion.Patellar Component (sometimes used)
Plastic surface replacing the kneecap underside.⸻
Step 5 — Alignment and Stability Check
The surgeon checks:
Motion
Implant fit
Alignment
Stability
Soft tissue balance
⸻
Step 6 — Closure
The incision is closed and recovery begins.
⸻
Surgical Approaches
Several surgical techniques may be used.
Traditional Total Knee Replacement
The most common approach.
Provides broad exposure and precise implant positioning.
Minimally Invasive Knee Replacement
Uses a smaller incision and less tissue disruption.
Potential benefits may include:
Less pain
Faster early recovery
Smaller scar
Not every patient is a candidate.
Robotic-Assisted Knee Replacement
Some surgeons use robotic systems to assist with:
Pre-operative planning
Bone preparation
Implant alignment
Precision balancing
Robotic assistance helps guide the surgeon but does not perform the surgery independently.
⸻
Benefits of Surgery
Potential benefits include:
Pain relief
Improved walking
Better range of motion
Increased independence
Improved sleep
Return to activities
Many patients report significant improvement in quality of life.
⸻
Risks of Surgery
Every surgery carries risk.
Possible complications include:
Infection
Blood clots
Bleeding
Implant loosening
Stiffness
Nerve or vessel injury
Persistent pain
Need for revision surgery
Your surgical team works to minimize these risks.
⸻
Recovery Overview
Most patients:
Stand or walk within 24 hours
Begin physical therapy quickly
Go home the same day or within several days
Improve steadily over weeks and months
Typical recovery:
Recovery Milestone
Timeline
Walking with assistance
Same day–1 day
Home recovery
1–2 weeks
Increased mobility
4–6 weeks
Return to many activities
6–12 weeks
Full recovery
3–12 months
Recovery varies by patient.
⸻
LDS Patient Message
Communication is the lifeline of care.
At Let’s Do Surgery, we help patients understand:
Why surgery may be needed
Which knee replacement options exist
What technology may be used
What recovery looks like
How to make informed decisions with their surgical team
We Don’t Just Inform — We Connect.
⸻
Professional-Facing Version
Total Knee Arthroplasty (TKA) — Clinical Procedure Overview
Definition
Total Knee Arthroplasty (TKA) is a reconstructive orthopedic procedure involving:
Resection of diseased articular surfaces
Restoration of mechanical alignment
Ligament balancing
Implantation of prosthetic femoral, tibial, and sometimes patellar components
Goal:
Pain relief
Functional restoration
Correction of deformity
Durable biomechanical reconstruction
⸻
Primary Indications
Degenerative Joint Disease
Most common indication.
Including:
End-stage osteoarthritis
Tricompartment disease
Bone-on-bone degeneration
Inflammatory Arthropathy
Examples:
Rheumatoid arthritis
Psoriatic arthritis
Chronic synovitis
Post-Traumatic Arthritis
Secondary to:
Fracture
Ligament instability
Meniscal loss
Prior surgery
Severe Deformity / Instability
Including:
Varus deformity
Valgus deformity
Flexion contracture
Multiplanar instability
⸻
Procedure Objectives
TKA seeks to achieve:
Mechanical Restoration
Neutral limb alignment
Joint line restoration
Proper component orientation
Soft Tissue Balance
Balanced:
Medial compartment
Lateral compartment
Flexion/extension gaps
Stable Kinematics
Goals include:
Functional ROM
Patellofemoral tracking
Stability throughout motion
⸻
Implant Construct
Typical construct:
Femoral Component
Usually:
Cobalt-chrome
Oxinium
Cemented or cementless
⸻
Tibial Baseplate
Options:
Metal tray
Cemented/cementless fixation
Stem augmentation if indicated
⸻
Polyethylene Insert
Designs:
Fixed-bearing
Mobile-bearing
Highly cross-linked polyethylene
⸻
Patellar Component
May be:
Resurfaced
Retained
Selectively resurfaced
Based on:
Surgeon preference
Cartilage status
Patient factors
⸻
Surgical Approaches
Common exposures:
Medial Parapatellar
Most widely utilized.
Advantages:
Excellent visualization
Familiar anatomy
Broad applicability
⸻
Midvastus / Subvastus
Muscle-sparing options.
Potential advantages:
Earlier quadriceps recovery
Reduced tissue disruption
Patient selection dependent.
⸻
Alignment Philosophy
Contemporary strategies include:
Mechanical Alignment
Traditional standard.
Goal:
Neutral hip-knee-ankle axis
⸻
Kinematic Alignment
Attempts to restore:
Native anatomy
Constitutional alignment
Physiologic ligament tension
⸻
Restricted Kinematic / Hybrid Strategies
Increasingly utilized.
Balance between:
Implant survivorship
Personalized alignment
⸻
Technology Integration
Modern TKA increasingly incorporates:
Computer Navigation
Enhances:
Alignment accuracy
Intraoperative measurements
⸻
Robotic-Assisted TKA
Examples may include:
Image-based systems
Imageless systems
Benefits:
Precision bone preparation
Gap balancing
Implant positioning
Reproducibility
⸻
Patient-Specific Instrumentation (PSI)
Uses:
CT/MRI-based planning
Customized cutting guides
Variable adoption.
⸻
Perioperative Pathway
Enhanced recovery pathways often include:
Preoperative Optimization
Glycemic control
Smoking cessation
Weight management
Medical clearance
Infection risk mitigation
Multimodal Analgesia
Common components:
Peripheral nerve block
Periarticular injection
NSAIDs
Acetaminophen
Limited opioid strategies
Early Mobilization
Goal:
Same-day ambulation
Accelerated rehabilitation
Reduced LOS
⸻
Outcome Expectations
Successful TKA commonly produces:
Significant pain reduction
Improved ROM
Functional restoration
High patient satisfaction
Long-term survivorship
Modern implants often demonstrate:
15–25+ year survivorship
High functional durability
Reduced revision rates with optimized technique and selection
⸻
LDS Professional Intelligence Positioning
The LDS Total Knee Module serves as a:
Decision Layer
Understanding:
Disease severity
Surgical candidacy
Implant and alignment strategy
Direction Layer
Matching:
Surgeon expertise
Technology availability
Facility capabilities
Connection Layer
Connecting:
Patients
Surgeons
Implant systems
Pharmaceutical and device support
Professional intelligence
Communication as the lifeline of care.
We Don’t Just Inform — We Connect. -
Total Knee Digital Module, Section 2: Anatomy module
Total Knee Digital Module
Section 2: Anatomy Module
Patient-Facing Version
What part of the body are we talking about?
A total knee replacement focuses on the knee joint, where the thigh bone, shin bone, and kneecap meet.
The knee works like a strong hinge that allows you to:
Walk
Stand
Climb stairs
Bend and straighten the leg
Support body weight
⸻
Main Knee Anatomy
1. Femur — Thigh Bone
The femur is the large bone of the upper leg.
The bottom end of the femur forms the top part of the knee joint.
In knee arthritis, the smooth surface at the end of the femur wears down.
During total knee replacement, the damaged end of the femur is reshaped and covered with a metal implant.
⸻
2. Tibia — Shin Bone
The tibia is the main bone of the lower leg.
It forms the bottom platform of the knee joint.
In surgery, the damaged top surface of the tibia is removed and replaced with a metal baseplate and plastic spacer.
⸻
3. Patella — Kneecap
The patella is the small bone in front of the knee.
It helps the thigh muscles straighten the leg.
Sometimes the back surface of the kneecap is resurfaced with a plastic button during knee replacement.
⸻
4. Cartilage — The Smooth Cushion
Cartilage is the smooth covering on the ends of the bones.
Healthy cartilage lets the knee glide smoothly.
In arthritis, cartilage wears away, causing:
Pain
Stiffness
Swelling
Bone-on-bone rubbing
Loss of motion
⸻
5. Meniscus — Shock Absorber
The knee has two menisci:
Medial meniscus — inside of the knee
Lateral meniscus — outside of the knee
They act like cushions between the femur and tibia.
In total knee replacement, these damaged cushioning structures are removed as part of joint resurfacing.
⸻
6. Ligaments — Knee Stabilizers
Ligaments are strong bands that hold the knee together.
Important knee ligaments include:
ACL — anterior cruciate ligament
PCL — posterior cruciate ligament
MCL — medial collateral ligament
LCL — lateral collateral ligament
In many total knee replacements, the ACL is removed.
The PCL may be kept or removed depending on implant design.
⸻
7. Muscles and Tendons
The main muscle group involved is the quadriceps, located in the front of the thigh.
The quadriceps connects to the patella and helps straighten the knee.
Other important structures include:
Quadriceps tendon
Patellar tendon
Hamstrings
Calf muscles
These muscles are important for walking, balance, and recovery after surgery.
⸻
Simple Patient Explanation
A total knee replacement does not replace the entire leg.
It replaces the damaged joint surfaces of the knee.
The surgeon removes worn-out cartilage and damaged bone from the:
Femur
Tibia
Sometimes patella
Then the knee is rebuilt using:
Metal components
Plastic spacer
Sometimes a plastic kneecap button
The goal is to create a smoother, more stable, less painful knee joint.
⸻
Professional-Facing Version
Core Anatomy for Total Knee Arthroplasty
Total knee arthroplasty addresses degenerative or damaged articular surfaces of the tibiofemoral and often patellofemoral compartments.
Key structures include:
Distal femur
Proximal tibia
Patella
Articular cartilage
Menisci
Collateral ligaments
Cruciate ligaments
Extensor mechanism
Neurovascular structures
⸻
Bony Anatomy
Distal Femur
Relevant landmarks:
Medial femoral condyle
Lateral femoral condyle
Intercondylar notch
Epicondyles
Posterior condyles
Trochlear groove
Femoral preparation must account for:
Mechanical axis
Femoral rotation
Posterior condylar axis
Epicondylar axis
Flexion-extension gap balance
⸻
Proximal Tibia
Relevant landmarks:
Medial tibial plateau
Lateral tibial plateau
Tibial spine region
Tibial tubercle
Posterior slope
Medial and lateral cortical boundaries
Tibial preparation focuses on:
Varus-valgus alignment
Posterior slope
Rotational alignment
Coverage without overhang
Balanced tibiofemoral contact
⸻
Patella
Important considerations:
Patellar thickness
Articular wear pattern
Tracking
Component positioning
Extensor mechanism tension
Patellar resurfacing depends on surgeon preference, implant system, cartilage status, and tracking.
⸻
Soft Tissue Anatomy
Ligaments
Key stabilizers:
MCL — primary medial restraint
LCL — lateral restraint
ACL — commonly sacrificed in TKA
PCL — retained or sacrificed depending on implant type
Implant choices may include:
Cruciate-retaining
Posterior-stabilized
Medial-stabilized
Constrained condylar
Hinged designs
⸻
Menisci
The medial and lateral menisci are removed during total knee arthroplasty as part of joint preparation.
Their load-sharing role is replaced by the polyethylene insert.
⸻
Extensor Mechanism
Includes:
Quadriceps muscle
Quadriceps tendon
Patella
Patellar tendon
Tibial tubercle
Protection of the extensor mechanism is critical for:
Postoperative function
Straight-leg raise
Stair climbing
Gait recovery
Patellar tracking
⸻
Neurovascular Anatomy
Important posterior structures include:
Popliteal artery
Popliteal vein
Tibial nerve
Common peroneal nerve laterally
Clinical relevance:
Posterior capsular work requires caution
Severe deformity increases neurovascular risk
Valgus knees require attention to peroneal nerve tension
Retractor placement is critical
⸻
Anatomy-Based Surgical Goals
The anatomy module should teach that total knee replacement is a surface replacement and alignment procedure.
The surgical goals are to:
Restore mechanical alignment
Balance flexion and extension gaps
Recreate stable knee motion
Maintain patellar tracking
Protect collateral ligaments
Preserve or substitute ligament function
Reduce painful bone-on-bone contact
⸻
LDS Visual Module Ideas
Interactive 3D Anatomy Map
Clickable structures:
Femur
Tibia
Patella
Cartilage
Meniscus
ACL/PCL
MCL/LCL
Quadriceps tendon
Patellar tendon
Patient Toggle
“Normal Knee” → “Arthritic Knee” → “Implanted Knee”
Professional Toggle
“Bone Cuts” → “Ligament Balance” → “Implant Position” → “Patellar Tracking”
Animation Sequence
Healthy knee joint
Cartilage wear begins
Bone-on-bone arthritis develops
Pain and deformity increase
Damaged surfaces are removed
Femoral and tibial implants are placed
Plastic spacer restores smooth motion
• 8. Knee bends and straightens with improved alignment
-
Total Knee Digital Module, Section 3: Disease states
Total Knee Digital Module
Section 3: Disease States
LDS Format — Patient Intelligence + Professional Intelligence Layer
Procedure Focus: Total Knee Arthroplasty (TKA / Total Knee Replacement)
⸻
SECTION 3 — DISEASE STATES
⸻
Patient-Facing Version
What Conditions Lead to Total Knee Replacement?
A Total Knee Replacement (TKA) is performed when the knee joint becomes damaged, painful, unstable, or worn down to the point that everyday activities become difficult and non-surgical treatments no longer provide relief.
The most common disease states include:
⸻
1. Osteoarthritis (OA)
“Wear-and-Tear Arthritis”
What is it?
Osteoarthritis is the most common reason for knee replacement.
It occurs when the cartilage cushioning the knee joint gradually wears away, allowing bone surfaces to rub against one another.
What happens in the knee?
Healthy knee:
Smooth cartilage
Easy motion
Minimal friction
Arthritic knee:
Cartilage loss
Bone-on-bone contact
Bone spur formation
Inflammation
Reduced motion
⸻
Common Symptoms
Knee pain
Stiffness
Swelling
Grinding or clicking
Difficulty climbing stairs
Trouble walking
Night pain
Limited motion
⸻
Risk Factors
Aging
Prior injury
Obesity
Genetics
Repetitive stress
Alignment problems
⸻
LDS Visual Layer
3D Animation:
Healthy knee → cartilage wear → bone-on-bone arthritis → knee replacement solution
⸻
2. Rheumatoid Arthritis (RA)
“Inflammatory Arthritis”
What is it?
Rheumatoid arthritis is an autoimmune disease.
The body’s immune system attacks the joint lining (synovium) causing inflammation and joint destruction.
⸻
What Happens?
Inflammation causes:
Synovial thickening
Cartilage damage
Bone erosion
Joint instability
Deformity
⸻
Symptoms
Often affects both knees.
Common findings:
Swelling
Warmth
Morning stiffness
Fatigue
Progressive pain
Reduced mobility
⸻
Why Surgery May Be Needed
When medications and biologic therapies fail to prevent joint destruction, TKA may restore:
Mobility
Alignment
Pain relief
Function
⸻
LDS Visual Layer
Immune attack animation:
Normal synovium → inflammation → cartilage erosion → deformity
⸻
3. Post-Traumatic Arthritis
“Arthritis After Injury”
What is it?
This arthritis develops after a knee injury.
Examples:
Fractures
Ligament tears
Meniscus injury
Sports trauma
Work injury
Even after healing, the joint may become arthritic years later.
⸻
Why Does It Happen?
Injury may cause:
Cartilage damage
Joint instability
Abnormal mechanics
Malalignment
Over time:
Accelerated wear
Chronic inflammation
Arthritis progression
⸻
Symptoms
Chronic pain
Swelling
Instability
Limited motion
Mechanical symptoms
⸻
LDS Visual Layer
Trauma timeline:
Injury → healing → altered mechanics → arthritis → replacement
⸻
4. Knee Deformity
“Alignment Problems”
Some patients develop severe deformity causing uneven pressure and progressive joint destruction.
Two common patterns:
⸻
Varus Knee
“Bow-Legged”
The knee angles outward.
Pressure concentrates on the:
Inner (medial) compartment
This is the most common arthritis pattern.
Symptoms:
Medial knee pain
Progressive bowing
Uneven walking
⸻
Valgus Knee
“Knock-Kneed”
The knee angles inward.
Pressure shifts to:
Outer (lateral) compartment
Symptoms:
Lateral pain
Instability
Difficulty walking
⸻
Why Replacement Helps
TKA restores:
Alignment
Joint balance
Weight distribution
Function
⸻
LDS Visual Layer
Interactive alignment comparison:
Normal vs Varus vs Valgus
⸻
5. Osteonecrosis (Avascular Necrosis)
“Bone Death from Loss of Blood Supply”
What is it?
Blood flow to part of the bone decreases or stops.
Without circulation:
Bone weakens
Bone collapses
Joint surface deteriorates
Often affects:
Femoral condyle
Tibial plateau
⸻
Risk Factors
Steroid use
Alcohol abuse
Trauma
Blood disorders
Sometimes unknown causes
⸻
Symptoms
Sudden pain
Progressive collapse
Swelling
Loss of function
⸻
When TKA is Needed
If collapse becomes severe and joint preservation fails.
⸻
LDS Visual Layer
Bone blood supply animation:
Normal perfusion → ischemia → collapse
⸻
6. Failed Previous Knee Surgery
“Revision or Salvage Arthritis”
Prior surgery may eventually fail.
Examples:
Failed cartilage procedures
Failed ligament reconstruction
Failed osteotomy
Partial knee failure
Hardware complications
These may lead to:
Progressive arthritis
Instability
Pain
Mechanical failure
⸻
Why TKA is Considered
Replacement may become the best reconstructive option.
⸻
LDS Visual Layer
Timeline:
Prior surgery → degeneration → reconstruction → TKA
⸻
7. Severe Cartilage Loss
“End-Stage Knee Degeneration”
Sometimes disease is less important than overall joint damage.
End-stage degeneration means:
Near complete cartilage loss
Bone-on-bone contact
Major pain
Functional disability
Patients often report:
Pain with every step
Reduced walking tolerance
Difficulty standing
Loss of independence
⸻
LDS Decision Point
TKA is typically considered when:
✔ Pain affects quality of life
✔ Walking and activity decline
✔ Conservative treatments fail
✔ Imaging confirms advanced disease
⸻
Professional-Facing Version
Disease State Intelligence Layer
⸻
Primary TKA Indications
Major etiologies:
Degenerative
Primary OA
Secondary OA
Post-meniscectomy OA
Inflammatory
RA
Psoriatic arthritis
Seronegative arthropathy
Post-Traumatic
Intra-articular fracture
Ligament instability
Malunion
Chronic overload
Structural
Varus deformity
Valgus deformity
Flexion contracture
Metabolic / Vascular
Osteonecrosis
Crystal arthropathy
Revision Pathology
Failed osteotomy
Failed unicompartmental arthroplasty
Hardware-associated degeneration
⸻
Radiographic Disease Patterns
Common findings:
OA
Joint-space narrowing
Osteophytes
Subchondral sclerosis
Cysts
Varus predominance
RA
Symmetric narrowing
Erosions
Osteopenia
Synovitis
Post-Traumatic
Irregular joint surface
Hardware
Malalignment
Focal degeneration
⸻
Disease Severity Assessment
Common scoring systems:
Clinical
WOMAC
KOOS
Oxford Knee Score
VAS Pain
SF-36
Radiographic
Kellgren–Lawrence
Ahlbäck
Mechanical axis evaluation
⸻
Professional Decision Layer
Disease state directly influences:
Implant selection
Constraint level
Soft tissue balancing
Bone defect strategy
Fixation method
Revision preparedness
Robotics/navigation use
Long-term survivorship planning
⸻
LDS Connection Layer
Disease → Decision → Direction → Connection
Disease state should guide:
Decision
Is surgery needed?
Joint preservation vs TKA?
Direction
Standard vs complex surgeon
Robotic vs conventional
Outpatient vs inpatient
Connection
Match patient with appropriate surgeon expertise and technology stack.
⸻
Section 3 LDS Output Summary
Patient Layer:
“What disease is damaging my knee and why do I need surgery?”
Professional Layer:
“How does disease pathology alter TKA planning, implants, alignment strategy, and outcomes?”
-
Total Knee Digital Module, Section 4: Pre-op workup
Total Knee Digital Module
Section 4: Pre-op Workup
Patient-facing version
Before a total knee replacement, your care team checks that surgery is the right choice, that your knee problem matches your symptoms, and that your body is ready for a safe operation and recovery.
1. Confirming the knee problem
Most patients have knee replacement because of severe knee arthritis. Your surgeon will review:
Your symptoms
Pain with walking, stairs, standing, or getting out of a chair
Stiffness or loss of motion
Swelling
Bow-legged or knock-kneed deformity
Pain that continues despite medicine, injections, therapy, or activity changes
Your imaging
Standing knee X-rays
Alignment views if needed
Sometimes MRI or CT if the diagnosis is unclear or custom/robotic planning is needed
2. Medical clearance
Your team checks whether your heart, lungs, kidneys, blood sugar, blood counts, and medications are safe for surgery.
Common pre-op tests may include:
Blood work
EKG
Chest X-ray if medically indicated
Urine testing if symptoms suggest infection
Primary care clearance
Cardiology clearance if you have heart disease
Dental or infection evaluation if there is concern for active infection
3. Medication review
Your team will review medications such as:
Blood thinners
Aspirin or anti-inflammatory drugs
Diabetes medicines
Blood pressure medicines
Steroids or immune-suppressing drugs
Opioid pain medications
Supplements that may increase bleeding risk
Some medications may need to be stopped or adjusted before surgery.
4. Infection prevention
Because an artificial knee implant is placed inside the body, preventing infection is a major focus.
Pre-op infection steps may include:
Skin cleansing instructions
Nasal screening for bacteria such as MRSA/MSSA
Antibiotics before surgery
Checking for open wounds, dental infection, urinary infection symptoms, or skin infection
Optimizing diabetes and nutrition
5. Physical preparation
The stronger and more flexible you are before surgery, the easier recovery may be.
Pre-op preparation may include:
“Prehab” physical therapy
Quadriceps strengthening
Range-of-motion exercises
Weight management if needed
Smoking cessation
Home safety planning
Walker/cane training
Planning transportation and help at home
6. Surgical planning
Your surgeon decides the safest and best plan for your knee.
Planning includes:
Implant type and size
Cemented vs cementless fixation
Robotic, computer-assisted, or conventional technique
Correcting alignment
Managing deformity or bone loss
Deciding whether outpatient or inpatient surgery is safest
7. Patient decision checklist
Before surgery, the patient should understand:
Why knee replacement is being recommended
What non-surgical treatments have been tried
What the implant does and does not do
Expected recovery timeline
Pain control plan
Risks and complications
Need for physical therapy
When they can walk, drive, return to work, and resume activities
⸻
Professional-facing version
The pre-op workup for total knee arthroplasty is designed to confirm indication, optimize modifiable risk factors, reduce infection and thromboembolic risk, support implant planning, and prepare the patient for postoperative rehabilitation.
1. Indication confirmation
Evaluate:
End-stage osteoarthritis, inflammatory arthritis, post-traumatic arthritis, avascular necrosis, or severe deformity
Failure of conservative management
Functional limitation affecting ADLs
Pain pattern consistent with radiographic disease
ROM limitation, flexion contracture, instability, varus/valgus deformity
Prior procedures, injections, infections, trauma, or hardware
2. Imaging workup
Standard imaging may include:
Weight-bearing AP knee X-ray
Lateral knee X-ray
Merchant/sunrise patellar view
Long-leg alignment films when deformity or mechanical-axis planning is needed
CT protocol for robotic/navigation/custom implant planning
MRI only when diagnosis is uncertain or soft-tissue pathology changes management
Assess:
Joint-space narrowing
Osteophytes
Subchondral sclerosis/cysts
Bone loss
Patellar tracking
Varus/valgus alignment
Flexion contracture
Prior hardware
Femoral/tibial bone quality
3. Medical optimization
Key optimization areas:
Cardiac risk assessment
Pulmonary risk assessment
Diabetes control
Renal function
Anemia correction
Nutritional status
BMI/weight optimization
Smoking cessation
Sleep apnea screening
History of DVT/PE
Chronic opioid use
Immunosuppression or inflammatory disease management
Common labs/tests:
CBC
CMP/BMP
PT/INR/PTT if indicated
HbA1c for diabetic or high-risk patients
Type and screen depending on institution
EKG based on age/risk
Additional testing guided by comorbidities
4. Infection-risk reduction
Pre-op infection protocol may include:
MRSA/MSSA nasal screening and decolonization
Chlorhexidine skin cleansing
Perioperative antibiotic plan
Dental infection evaluation when clinically indicated
Delay surgery for active skin wounds, cellulitis, systemic infection, or symptomatic UTI
Glycemic optimization
Nutrition/protein optimization
Smoking cessation
Avoidance of intra-articular steroid injection close to surgery per institutional policy
5. Medication management
Review and coordinate:
Anticoagulants: warfarin, DOACs, heparins
Antiplatelets: aspirin, clopidogrel
NSAIDs
Diabetes agents, including insulin and GLP-1 medications
Steroids and biologics
Rheumatologic medications
Chronic opioids
Supplements affecting bleeding
Hormonal therapy if VTE risk is relevant
Medication decisions should be coordinated with anesthesia, primary care, cardiology, or prescribing specialists.
6. VTE risk planning
Assess:
Prior DVT/PE
Cancer history
Thrombophilia
Obesity
Limited mobility
Hormone therapy
Smoking
Bilateral procedures
Revision or complex surgery
Plan:
Mechanical prophylaxis
Early mobilization
Chemoprophylaxis selection
Duration of prophylaxis
Outpatient vs inpatient monitoring needs
7. Anesthesia and pain pathway
Pre-op anesthesia review includes:
General vs spinal/regional anesthesia
Peripheral nerve block plan
Multimodal pain protocol
Opioid-sparing strategy
Nausea prevention
Sleep apnea precautions
Post-op monitoring needs
Common multimodal components may include acetaminophen, NSAID/COX-2 inhibitor when appropriate, regional blocks, periarticular injection, and limited opioid rescue.
8. Implant and technical planning
Surgeon planning includes:
Implant system
Cruciate-retaining vs posterior-stabilized vs medial-pivot/constrained design
Cemented vs cementless fixation
Patellar resurfacing decision
Polyethylene thickness options
Alignment philosophy: mechanical, kinematic, restricted kinematic, or functional alignment
Robotic/navigation/manual instrumentation
Management of varus/valgus deformity
Ligament balancing strategy
Bone defects and augments if needed
Prior hardware removal strategy
Tourniquet use
Blood conservation plan
9. Discharge planning
Determine whether the patient is appropriate for same-day discharge, short-stay admission, or inpatient rehab.
Assess:
Home support
Stairs and home layout
Baseline mobility
Cognitive status
Fall risk
Transportation
Access to outpatient or home PT
Medical comorbidity burden
Patient expectations and motivation
10. LDS pre-op intelligence checklist
Decision layer
Is TKA truly indicated?
Has conservative care failed?
Does imaging match symptoms?
Does the patient understand alternatives?
Direction layer
Is the patient suited for outpatient or inpatient TKA?
Does the surgeon/hospital have the needed technology?
Is robotic or navigation planning useful?
Are complex-case resources needed?
Connection layer
Which implant/device pathway is being used?
Are reps needed for implant system support?
Are special trays, robotics, cementless components, augments, or constrained implants required?
Is the patient connected to education, rehab, and follow-up resources?
Section 4 Output Summary
The pre-op workup is the safety and planning phase of total knee replacement. It confirms the diagnosis, prepares the patient medically, reduces infection and clot risk, supports implant selection, and creates the recovery plan before the patient enters the operating room.
-
Total Knee Digital Module, Section 5: Procedure approaches
Total Knee Digital Module
Section 5: Procedure Approaches
Patient-Facing Version
A total knee replacement can be performed using different surgical approaches and technologies. The goal is the same: remove damaged joint surfaces and replace them with artificial components that help reduce pain, improve alignment, and restore movement.
Main Procedure Approaches
1. Traditional Total Knee Replacement
This is the standard approach.
The surgeon makes an incision over the front of the knee, moves soft tissue aside, removes damaged cartilage and bone, and places metal and plastic implants.
Best for:
Most patients with advanced arthritis, deformity, stiffness, or severe pain.Key points:
Reliable, widely used, predictable outcomes.⸻
2. Minimally Invasive Total Knee Replacement
This uses a smaller incision and less soft-tissue disruption.
The goal is to reduce trauma to muscles and tendons while still placing the implant accurately.
Best for:
Selected patients with good bone structure, less severe deformity, and appropriate anatomy.Key points:
May allow less pain early on, faster early recovery, but not right for everyone.⸻
3. Robotic-Assisted Total Knee Replacement
A robotic system helps the surgeon plan and perform bone cuts with high precision.
The surgeon remains in control, but the robot assists with alignment, balancing, and implant positioning.
Best for:
Patients who may benefit from customized alignment, precise implant placement, or complex anatomy.Key points:
Improves planning and accuracy. It does not replace the surgeon.⸻
4. Computer-Navigated Total Knee Replacement
This uses sensors and imaging guidance to help the surgeon align the knee implant.
It works like GPS for the knee, helping guide bone cuts and implant position.
Best for:
Patients where alignment is especially important, including deformity or prior surgery.Key points:
Helps improve accuracy without necessarily using a robotic arm.⸻
5. Patient-Specific Instrumentation
Preoperative imaging is used to create custom cutting guides for the patient’s knee.
These guides help the surgeon make planned bone cuts based on the patient’s anatomy.
Best for:
Patients where customized planning may improve efficiency or alignment.Key points:
Uses pre-surgery imaging and customized guides.⸻
Implant Design Options
Cruciate-Retaining Knee
The surgeon keeps the patient’s posterior cruciate ligament if it is healthy.
Posterior-Stabilized Knee
The posterior cruciate ligament is removed and replaced by a mechanical stabilizing design in the implant.
Constrained Knee
Used when ligaments are weak or unstable.
Hinged Knee
Used in complex revision cases, severe deformity, or major ligament loss.
⸻
Patient Decision Support
Patients should ask:
Which approach is best for my knee condition?
Do I need robotic or computer-assisted technology?
What implant design will be used?
How much arthritis, deformity, or ligament damage do I have?
What recovery timeline should I expect?
⸻
Professional-Facing Version
Procedure Approach Categories
1. Conventional Manual TKA
Standard exposure with manual instrumentation, intramedullary femoral and extramedullary tibial alignment guides.
Use cases:
Primary OA, RA, post-traumatic arthritis, standard varus/valgus deformity.Key considerations:
Alignment philosophy, ligament balancing, bone quality, flexion-extension gap symmetry.⸻
2. Minimally Invasive TKA
Smaller incision with quadriceps-sparing or mid-vastus/subvastus variations.
Advantages:
Reduced early soft-tissue trauma, potential faster early functional gains.Limitations:
Reduced visualization, risk of component malposition if exposure is inadequate.⸻
3. Robotic-Assisted TKA
Preoperative CT-based or imageless planning depending on platform.
Core benefits:
Precision bone preparation, implant sizing, real-time gap balancing, controlled resection boundaries.Clinical value:
Especially useful in complex alignment, deformity, obesity, prior hardware, or customized kinematic planning.⸻
4. Computer-Navigated TKA
Uses optical trackers, sensors, or navigation arrays to guide alignment and bone cuts.
Applications:
Mechanical axis correction, component rotation, deformity cases, retained hardware where intramedullary guides are difficult.⸻
5. Patient-Specific Instrumentation
Preoperative MRI or CT used to create custom cutting blocks.
Potential benefits:
Preoperative templating, reduced instrument trays, improved workflow.Limitations:
Accuracy depends on imaging, planning, guide fit, and intraoperative validation.⸻
Surgical Exposure Options
Medial Parapatellar Approach
Most common approach. Provides broad exposure and reliable visualization.
Midvastus Approach
Splits vastus medialis fibers. May preserve quadriceps mechanism better.
Subvastus Approach
Avoids cutting quadriceps tendon. Technically more demanding.
Quadriceps-Sparing Approach
Least invasive soft-tissue approach, but limited exposure and steep learning curve.
⸻
Alignment Philosophies
Mechanical Alignment
Restores neutral mechanical axis.
Anatomical Alignment
Attempts to recreate native joint line orientation.
Kinematic Alignment
Attempts to restore the patient’s pre-arthritic knee anatomy.
Functional Alignment
Uses robotic/navigation data to balance alignment, soft tissue tension, and implant position.
⸻
Implant Constraint Selection
Implant Type
Indication
Cruciate-retaining
Intact PCL, good ligament balance
Posterior-stabilized
PCL deficiency or surgeon preference
Medial pivot
Designed to mimic medial stability
Varus-valgus constrained
Collateral ligament insufficiency
Rotating hinge
Severe instability, revision, tumor, major bone loss
⸻
LDS Procedure Builder Logic
The module should allow users to compare:
Approach:
Manual vs minimally invasive vs robotic-assisted vs navigation-assisted vs patient-specific.Exposure:
Medial parapatellar vs midvastus vs subvastus vs quadriceps-sparing.Alignment strategy:
Mechanical vs kinematic vs functional.Implant design:
CR vs PS vs medial pivot vs constrained vs hinged.Technology layer:
Robotic arm, navigation, smart sensors, pressure balancing, patient-specific guides.Patient factors:
Age, BMI, activity level, deformity, bone quality, ligament stability, prior surgery, inflammatory arthritis.⸻
LDS Summary Statement
Total knee replacement is not one single procedure. It is a customizable surgical build.
The best approach depends on the patient’s anatomy, arthritis pattern, ligament stability, deformity, activity goals, implant selection, and the technology available to the surgical team. -
Total Knee Digital Module, Section 6: Step-by-step workflow
Total Knee Digital Module
Section 6: Step-by-Step Workflow
Patient-Facing Version + Professional-Facing Version
LDS Framework: Communication as the Lifeline of Care
⸻
PATIENT-FACING VERSION
What Happens During a Total Knee Replacement?
Your Step-by-Step Surgical Journey
A Total Knee Replacement (Total Knee Arthroplasty / TKA) is performed to remove damaged joint surfaces and replace them with artificial components designed to restore movement, relieve pain, and improve function.
Most procedures take 60–120 minutes, depending on anatomy, deformity, previous surgery, and technology used.
⸻
Step 1: Preoperative Preparation
Before surgery:
You arrive at the hospital or surgery center
The surgical team will:
• Confirm your identity and procedure
• Review imaging and surgical plan
• Verify allergies and medications
• Start an IV line
• Mark the operative knee
You will meet:
• Orthopedic surgeon
• Anesthesia team
• Nursing staff
• Surgical support team
Common preparation includes:
• Blood pressure and vital signs
• Antibiotics to reduce infection risk
• Compression devices for clot prevention
• Surgical site cleansing
LDS Voice Prompt:
“Today we are replacing your damaged knee joint to reduce pain and help restore mobility.”
⸻
Step 2: Anesthesia
Most knee replacements are performed using:
Regional anesthesia (common)
Often a spinal block combined with sedation.
Benefits may include:
• Less nausea
• Better pain control
• Reduced opioid use
• Faster recovery
General anesthesia
Sometimes used depending on patient condition or surgeon preference.
You will not feel pain during surgery.
⸻
Step 3: Positioning and Sterile Setup
You are positioned safely on the operating table.
The team:
• Pads pressure points
• Positions the operative leg
• Cleans the knee with antiseptic solution
• Applies sterile drapes
This creates a protected sterile environment.
⸻
Step 4: Surgical Incision
The surgeon makes an incision over the front of the knee.
Typical incision:
• Midline incision
• Approximately 4–10 inches
• Size depends on anatomy and technique
The knee joint is carefully exposed while protecting muscles, ligaments, and surrounding tissues.
⸻
Step 5: Joint Exposure
The kneecap (patella) is gently moved aside to access the joint.
The surgeon evaluates:
• Cartilage damage
• Bone wear
• Arthritis severity
• Joint alignment
• Ligament balance
This confirms the surgical plan.
⸻
Step 6: Removal of Damaged Bone and Cartilage
The damaged joint surfaces are removed.
This includes:
Distal femur
Lower end of the thigh bone.
Proximal tibia
Top of the shin bone.
Sometimes the patella
Depending on surgeon preference and patient anatomy.
Special guides or robotic systems help ensure precision.
⸻
Step 7: Bone Preparation and Alignment
The remaining bone is shaped to accept the implants.
Goal:
• Restore alignment
• Improve motion
• Balance the joint
• Create stable implant fixation
Technology may include:
• Manual instrumentation
• Computer navigation
• Robotic assistance
The surgeon repeatedly checks movement and stability.
⸻
Step 8: Trial Components
Temporary trial implants are placed.
The surgeon tests:
• Knee flexion and extension
• Stability
• Implant sizing
• Ligament tension
• Walking mechanics
This helps confirm the best fit before final implantation.
⸻
Step 9: Final Implant Placement
Permanent components are inserted.
Typical implants include:
Femoral component
Metal surface replacing damaged femur.
Tibial component
Metal base attached to tibia.
Polyethylene liner
Smooth plastic surface creating gliding motion.
Patellar component (sometimes)
Resurfacing of kneecap.
Fixation may use:
• Bone cement
• Cementless fixation
• Hybrid techniques
⸻
Step 10: Final Motion and Stability Check
Before closing, the surgeon confirms:
• Alignment
• Range of motion
• Stability
• Implant tracking
• Patellar movement
• Bleeding control
The knee is moved through its full range.
⸻
Step 11: Closure
The knee is closed in layers.
Closure may include:
• Sutures
• Staples
• Absorbable materials
• Surgical adhesive
Dressings are applied.
Some surgeons use:
• Compression wraps
• Cryotherapy systems
• Negative-pressure dressings
⸻
Step 12: Recovery Room (PACU)
After surgery:
You move to the Post-Anesthesia Care Unit (PACU).
The team monitors:
• Pain
• Blood pressure
• Oxygen
• Circulation
• Knee function
Many patients begin moving the knee and standing within hours.
⸻
Step 13: Early Mobilization and Rehabilitation
Movement starts early.
Goals:
• Walking
• Knee bending
• Strength recovery
• Prevent blood clots
• Restore independence
Physical therapy is critical.
Typical milestones:
Day 0–1: Standing and walking
Week 2–6: Improved motion and strength
Month 2–3: Return to many activities
Month 3–12: Continued healing and functional improvement
⸻
PROFESSIONAL-FACING VERSION
Total Knee Arthroplasty (TKA) Surgical Workflow
⸻
1. Preoperative Planning
Review:
• Weight-bearing radiographs
• Alignment
• Mechanical axis
• Implant templating
• Bone loss
• Deformity
• Ligament status
Technology planning:
• Conventional
• Computer-assisted
• Robotic workflow
Pre-op considerations:
• Infection screening
• VTE risk
• Medical optimization
• ERAS pathway
⸻
2. Anesthesia and Regional Block
Common strategies:
• Spinal anesthesia
• Adductor canal block
• IPACK block
• General anesthesia when indicated
Goals:
• Multimodal pain control
• Early ambulation
• Reduced opioid exposure
⸻
3. Positioning and OR Setup
Typical setup:
• Supine position
• Tourniquet optional
• Leg holder or padded bump
• Knee flexion capability >120°
Equipment:
• Power instruments
• Navigation/robotics if used
• Cement preparation
• Pulse lavage
• Implant trays
⸻
4. Surgical Exposure
Common approach:
Medial parapatellar arthrotomy
Alternatives:
• Midvastus
• Subvastus
• Quadriceps-sparing
Goals:
• Adequate visualization
• Soft tissue preservation
• Safe exposure
⸻
5. Femoral and Tibial Preparation
Bone resections performed using:
Conventional guides
Intramedullary or extramedullary alignment.
Navigation/robotics
Real-time planning and precision execution.
Resections:
• Distal femur
• Proximal tibia
• Femoral sizing/cuts
⸻
6. Gap Balancing and Soft Tissue Management
Critical workflow phase.
Assess:
• Extension gap
• Flexion gap
• Coronal balance
• Rotational alignment
Potential releases:
• MCL
• Posteromedial capsule
• IT band
• Lateral structures in valgus knees
Goal:
Balanced, stable knee through ROM.
⸻
7. Trial Reduction
Trial evaluation:
• Component sizing
• Tracking
• ROM
• Stability
• Patellar mechanics
• Flexion-extension symmetry
Decision points:
• Polyethylene thickness
• Constraint level
• Alignment modifications
⸻
8. Implant Fixation
Implant strategies:
Cemented
Most common.
Cementless
Increasing use in selected patients.
Hybrid
Selective fixation.
Critical considerations:
• Bone quality
• Cement mantle
• Press-fit stability
⸻
9. Patellar Management
Approaches:
• Resurfacing
• Selective resurfacing
• Retention
Assess:
• Tracking
• Thickness
• Tilt
• Subluxation
⸻
10. Final Assessment and Hemostasis
Confirm:
• Mechanical alignment
• Stability
• Tracking
• ROM
• Bleeding control
Adjuncts:
• Pulse lavage
• Hemostatic agents
• TXA protocols
⸻
11. Closure
Layered closure:
• Arthrotomy
• Deep tissue
• Subcutaneous layer
• Skin
Options:
• Staples
• Running absorbable closure
• Barbed sutures
• Skin adhesive
⸻
12. Postoperative Pathway
ERAS goals:
• Same-day or short stay
• Multimodal analgesia
• Early PT
• VTE prophylaxis
• Rapid functional recovery
Standard monitoring:
• Neurovascular status
• Pain control
• Wound integrity
• Mobility milestones
⸻
LDS Visual / Interactive Layer Recommendations
For the Total Knee Step-by-Step Workflow Module, include:
Patient Layer
• 3D animated knee replacement surgery
• “Day in the Life of Knee Replacement” walkthrough
• Voice-guided surgery explanation
• Recovery timeline animation
Professional Layer
• Robotic vs conventional TKA workflow toggle
• Implant positioning simulator
• Gap balancing visualization
• Ligament tension and alignment overlays
• OR setup and instrument mapping module
LDS Principle:
We Don’t Just Inform — We Connect.
This workflow explains not only what happens during knee replacement, but why each surgical step matters to patient outcomes and procedural success.
-
Total Knee Digital Module, Section 7: Critical View of Safety module
Total Knee Digital Module
Section 7: Critical View of Safety Module
1. What “Critical View of Safety” Means in Total Knee Replacement
In gallbladder surgery, the Critical View of Safety confirms anatomy before cutting.
In Total Knee Arthroplasty, the safety equivalent is:
Confirm the knee is correctly aligned, balanced, stable, tracking, and safely implanted before final components are placed.
This is the TKA Safety View.
⸻
Patient-Facing Version
The surgeon checks 5 major safety points
1. Is the leg straight?
The surgeon checks that the new knee restores proper leg alignment.
2. Is the knee balanced?
The inside and outside ligaments must feel even, not too tight or too loose.
3. Does the knee bend and straighten smoothly?
The surgeon tests motion before the final implant is placed.
4. Does the kneecap track correctly?
The kneecap should glide smoothly in the center of the knee.
5. Are the trial implants stable?
Temporary trial pieces are tested before the permanent implants are inserted.
⸻
Professional-Facing Version
TKA Critical Safety Checkpoints
1. Alignment Confirmation
Confirm coronal, sagittal, and rotational alignment of femoral and tibial components. TKA success depends heavily on limb alignment, component positioning, ligament stability, ROM, and patellar tracking.
2. Extension Gap Assessment
Verify full extension without recurvatum or flexion contracture.
3. Flexion Gap Assessment
Confirm balanced medial/lateral gaps at 90° flexion.
4. Ligament Balance
Evaluate MCL/LCL tension, varus-valgus stability, and flexion-extension symmetry.
5. Tibial Rotation
Confirm tibial tray rotation using anatomic landmarks and trial tracking.
6. Femoral Rotation
Avoid internal rotation; confirm balanced flexion gap and patellofemoral tracking.
7. Patellar Tracking
Assess central tracking through ROM before closure.
8. Trial Reduction
Test ROM, stability, rollback, patellar behavior, and implant sizing before cementation/final fixation.
⸻
LDS “Do Not Proceed” Safety Rules
Do not implant final components until:
Alignment is acceptable
Flexion and extension gaps are balanced
Knee is stable in extension, mid-flexion, and flexion
Patella tracks properly
Trial implants move smoothly
No major instability, malrotation, or impingement is present
⸻
Visual Module Concept
Interactive Safety Dashboard
Green = Safe to Proceed
Yellow = Adjust / Recheck
Red = Do Not Proceed
Dashboard Tiles
Alignment
Bone cuts
Extension gap
Flexion gap
Ligament balance
Tibial rotation
Femoral rotation
Patellar tracking
Trial ROM
Final implant readiness
⸻
LDS Voiceover Script
“Before the final knee replacement implants are placed, the surgeon performs a safety check. The leg alignment is checked, the ligaments are balanced, the knee is moved through a full range of motion, and the kneecap is observed to make sure it tracks smoothly. This step helps reduce the risk of stiffness, instability, pain, implant wear, and revision surgery.”
⸻
Section 7 Summary
The Critical View of Safety in Total Knee Replacement is not one single view.
It is a multi-step confirmation system:
Align the limb. Balance the ligaments. Test the motion. Confirm the tracking. Then implant.
-
Total Knee Digital Module, Section 8: Device and supply stack
Total Knee Digital Module
Section 8: Device and Supply Stack
LDS Format – Patient Intelligence + Professional Intelligence Layer
⸻
PATIENT-FACING VERSION
What Devices and Supplies Are Used in a Total Knee Replacement?
A Total Knee Replacement (Total Knee Arthroplasty – TKA) is performed using a carefully coordinated set of medical devices, implants, surgical instruments, and sterile supplies.
Think of the procedure like a precision-engineered reconstruction of the knee joint.
The surgeon removes damaged cartilage and bone and replaces them with specially designed implants that restore motion, alignment, and function.
⸻
1. Core Implant Components
A total knee replacement typically contains three primary implant components.
A. Femoral Component (Thigh Bone Implant)
This metal implant covers the end of the femur.
Purpose:
Replaces damaged cartilage
Restores smooth joint motion
Forms the top half of the new knee
Typical Materials:
Cobalt-chromium alloy
Titanium alloy
Oxidized zirconium (selected systems)
⸻
B. Tibial Component (Shin Bone Implant)
This implant sits on the top of the tibia.
Usually includes:
Metal Baseplate
+
Plastic Insert
Purpose:
Creates stable weight-bearing surface
Supports motion
Transfers body load
⸻
C. Polyethylene Insert (Spacer)
The spacer sits between metal components.
Purpose:
Acts as cartilage substitute
Reduces friction
Provides shock absorption
Allows smooth flexion and extension
Material:
Highly Cross-Linked Polyethylene (HXLPE)
⸻
D. Patellar Component (Optional)
Some surgeons resurface the kneecap.
This may involve:
Polyethylene button
Patellar implant
Purpose:
Improve patellar tracking
Reduce anterior knee pain
Create smoother motion
⸻
2. Implant Design Options
Not every knee replacement is built the same.
Surgeons select implant design based on:
Anatomy
Ligament stability
Bone quality
Deformity
Activity level
⸻
Posterior Stabilized (PS)
Uses a cam-post mechanism.
When Used:
PCL removed
Added stability needed
Advantages
Predictable motion
Good flexion
⸻
Cruciate Retaining (CR)
Preserves posterior cruciate ligament.
When Used:
Intact PCL
Stable knee
Advantages
More natural knee mechanics
⸻
Constrained / Hinged Systems
Used in complex cases.
Examples:
Severe deformity
Revision surgery
Major instability
⸻
3. Surgical Navigation and Technology
Modern TKA increasingly uses technology for precision.
⸻
Robotic-Assisted TKA
Robotic systems help surgeons:
Plan bone cuts
Improve implant alignment
Balance ligaments
Increase precision
Examples include:
Robotic arm platforms
CT-based planning systems
Image-guided systems
Patients should understand:
The robot does not perform surgery alone.
The surgeon remains in full control.
⸻
Computer Navigation
Provides real-time positioning data.
Purpose:
Alignment guidance
Bone cut accuracy
Mechanical axis restoration
⸻
Smart Instrumentation
Includes:
Digital tensioning systems
Gap balancing tools
Sensor-assisted devices
Goal:
Create balanced motion and stability.
⸻
4. Surgical Instrument Stack
The implant cannot be placed without a specialized instrument system.
⸻
Cutting Guides
Precision guides determine:
Bone resection depth
Alignment
Rotation
⸻
Alignment Rods
Help orient implants relative to leg axis.
⸻
Trial Components
Temporary implants used during surgery.
Purpose:
Confirm size
Test motion
Check stability
Evaluate ligament balance
⸻
Bone Preparation Instruments
Used to shape bone.
Examples:
Oscillating saw
Burrs
Reamers
Punches
Rongeurs
⸻
Cement Delivery System
If cemented fixation used:
Supplies include:
Vacuum mixer
Cement gun
Pressurization tools
⸻
5. Fixation Materials
Implants must attach securely to bone.
Two primary methods exist.
⸻
Cemented Fixation
Most common.
Uses:
PMMA Bone Cement
Purpose:
Immediate fixation
Reliable stability
Widely used
⸻
Cementless Fixation
Implant surface designed for bone ingrowth.
Features:
Porous coating
Biologic fixation
More common in:
Younger patients
Good bone quality
⸻
6. Sterile Disposable Supply Stack
Every TKA uses a large sterile support system.
Typical supplies:
Access + Exposure
Drapes
Towels
Skin prep
Retractors
Suction tubing
Hemostasis
Electrocautery pencils
Smoke evacuation
Tourniquet systems
Closure Supplies
Sutures
Staples
Adhesives
Dressings
Irrigation
Sterile saline
Pulse lavage systems
⸻
7. Imaging and OR Equipment
Operating room equipment supports accuracy and safety.
Typical equipment:
OR table
Positioners
Surgical lights
Power systems
Sterile instrument trays
Implant inventory
Imaging systems (selected cases)
⸻
PROFESSIONAL-FACING VERSION
Total Knee Device and Supply Intelligence Layer
The TKA device stack functions as an integrated procedural ecosystem.
⸻
Implant System Layer
Major implant manufacturers frequently include:
Zimmer Biomet
Stryker
DePuy Synthes
Smith & Nephew
Exactech
MicroPort
Typical implant categories:
Femoral Components
CoCr
Titanium
Oxinium variants
Tibial Baseplates
Cemented
Porous-coated
Keel or stem options
Inserts
Conventional PE
HXLPE
Vitamin-E stabilized PE
⸻
Instrumentation Layer
Procedural sets commonly include:
Standard Instrument Sets
Distal femoral guides
Tibial cutting blocks
Intramedullary/Extramedullary guides
Trialing systems
Patient-Specific Instrumentation (PSI)
May use:
MRI/CT planning
Disposable custom guides
⸻
Robotic / Digital Layer
Technology platforms increasingly integrated.
Examples:
Robotic
MAKO
ROSA
VELYS
Navigation
Optical
Accelerometer-based
CT-enabled
Capabilities:
Gap balancing
Kinematic planning
Alignment analytics
Ligament tension mapping
⸻
Pharmaceutical + Device Interaction Layer
Section 8 interfaces closely with:
Section 9 – Pharma Layer
Typical interactions:
Antibiotic cement
Tranexamic acid protocols
Local anesthetic infiltration
Hemostasis protocols
⸻
LDS Procedure Builder Integration
Within the Let’s Do Surgery Procedure Builder, the TKA stack can become selectable and configurable.
Example:
Build Your Knee Replacement
Implant
CR
PS
Constrained
Fixation
Cemented
Cementless
Hybrid
Technology
Conventional
Navigation
Robotic
Patella
Resurface
Preserve
Manufacturer
User selectable
Surgeon preference
Facility inventory
⸻
LDS Connection Layer
Device stack transparency creates connection opportunities between:
Patient ↔ Surgeon ↔ Device Representative ↔ Facility
Potential LDS overlays:
Implant technology explanations
Manufacturer profiles
Robotics availability
Facility inventory mapping
Rep support integration
Procedure Builder comparison tools
⸻
LDS Core Message
We Don’t Just Inform — We Connect.
The Total Knee device and supply stack is not simply a list of tools — it is the engineered system that allows a surgeon to restore movement, reduce pain, and personalize care for each patient.
Visualization
• laparoscope
• camera head
• light source
• insufflator
Dissection
• Maryland dissector
• hook cautery
• blunt grasper
• atraumatic grasper
• suction irrigator
Hemostasis / division
• clip applier
• laparoscopic clips
• energy device if used
Specimen handling
• endoscopic retrieval bag
Closure
• fascial closure device
• sutures
• skin adhesive / steri-strips / staples
LDS feature:
Every step opens the relevant devices, manufacturers, SKU fields, rep contacts, and preference-card notes.
-
Total Knee Digital Module, Section 9: Pharma layer
Total Knee Digital Module
Section 9: Pharma Layer
LDS Framework | Patient Intelligence + Professional Intelligence
⸻
SECTION 9A: Patient-Facing Version
Pharmaceutical Support During Total Knee Replacement (TKR)
Why Medications Matter in Knee Replacement Surgery
A Total Knee Replacement (TKR) is not only a mechanical procedure involving implants and surgical tools—it is also supported by carefully selected medications that help patients:
Prevent infection
Control pain
Reduce inflammation
Prevent blood clots
Manage nausea
Support healing and recovery
The medication plan begins before surgery, continues during the operation, and extends into recovery at home.
⸻
1. Preoperative Medications (Before Surgery)
These medications prepare the body for surgery and improve outcomes.
Antibiotics
Given before incision to prevent infection.
Common examples:
Cefazolin (Ancef)
Clindamycin
Vancomycin
Purpose:
Reduce surgical site infection risk
Protect implant from bacterial contamination
⸻
Pain Preparation (Preemptive Analgesia)
Pain medications may be given before surgery to reduce postoperative discomfort.
Common medications:
Acetaminophen (Tylenol)
Celecoxib (Celebrex)
Gabapentin or Pregabalin
Purpose:
Lower pain signals before surgery begins
Reduce opioid requirements later
⸻
Anxiety / Sedation Medication
Patients may receive light sedation before entering the OR.
Examples:
Midazolam (Versed)
Purpose:
Relaxation
Anxiety reduction
Improved comfort
⸻
2. Intraoperative Medications (During Surgery)
These medications support the surgical procedure.
⸻
Anesthesia
TKR may be performed under:
Spinal Anesthesia
Common for knee replacement.
Benefits:
Less nausea
Lower opioid use
Faster recovery
Lower blood loss
Medications:
Bupivacaine
Lidocaine
⸻
General Anesthesia
Patient fully asleep.
Common medications:
Propofol
Sevoflurane
Fentanyl
⸻
Regional Nerve Blocks
Many patients receive targeted pain blocks.
Common blocks:
Adductor Canal Block
Femoral Nerve Block
IPACK Block
Typical medications:
Ropivacaine
Bupivacaine
Purpose:
Numb knee region
Improve early mobility
Reduce opioid use
⸻
Tranexamic Acid (TXA)
A major medication in modern TKR.
Purpose:
Reduce bleeding
Lower transfusion rates
Improve recovery
Benefits:
Less blood loss
Reduced swelling
Faster rehabilitation
⸻
Antibiotic Redosing
Long surgeries may require additional antibiotic dosing.
Goal:
Maintain sterile protection throughout surgery
⸻
3. Postoperative Medications (Recovery Phase)
After surgery, medications focus on pain control and safe recovery.
⸻
Pain Control
Modern TKR uses multimodal pain management.
This means using several medications together rather than relying on opioids alone.
Common medications:
Non-opioid Pain Relief
Acetaminophen
Celecoxib
Ketorolac (Toradol)
Purpose:
Reduce inflammation
Improve comfort
Minimize narcotic need
⸻
Opioids (Short-Term Use)
Used when stronger pain relief is needed.
Examples:
Oxycodone
Hydrocodone
Morphine
Purpose:
Severe pain control
Important:
Usually temporary
Goal is early reduction
⸻
Blood Clot Prevention (DVT Prophylaxis)
Knee replacement increases risk of:
Deep Vein Thrombosis (DVT)
Pulmonary Embolism (PE)
Common medications:
Aspirin
Enoxaparin (Lovenox)
Apixaban (Eliquis)
Rivaroxaban (Xarelto)
Purpose:
Prevent dangerous blood clots
⸻
Anti-Nausea Medications
Help prevent postoperative nausea.
Examples:
Ondansetron (Zofran)
Dexamethasone
Purpose:
Improve comfort
Encourage eating and walking
⸻
Constipation Prevention
Pain medications may slow bowel function.
Common support:
Docusate
Senna
Polyethylene glycol (Miralax)
Goal:
Maintain normal bowel activity
⸻
Patient Medication Timeline
Surgery Phase
Medication Goal
Before Surgery
Prevent infection + prepare for pain
During Surgery
Anesthesia + bleeding + comfort
Immediately After
Pain + nausea + mobility
Home Recovery
Healing + clot prevention + taper pain meds
⸻
LDS Patient Insight
The implant replaces the knee—but medications help the body safely accept and recover from the surgery.
Successful TKR depends on:
Implant + Surgery + Medication Strategy + Rehabilitation
⸻
SECTION 9B: Professional-Facing Version
Professional Pharma Intelligence Layer – Total Knee Arthroplasty (TKA)
⸻
1. Perioperative Pharmaceutical Architecture
Modern TKA pharma strategy focuses on:
Enhanced Recovery After Surgery (ERAS)
Goals:
Opioid reduction
Early ambulation
Shortened LOS
Reduced complications
Improved patient satisfaction
⸻
2. Standard Perioperative Drug Categories
Category
Purpose
Examples
Antibiotics
Infection prevention
Cefazolin, Vancomycin
Analgesics
Pain control
Acetaminophen, NSAIDs
Regional anesthesia
Sensory blockade
Ropivacaine
Antifibrinolytics
Blood conservation
TXA
Anticoagulants
DVT prevention
Aspirin, DOACs
Steroids
Inflammation + nausea
Dexamethasone
Opioids
Rescue analgesia
Oxycodone
GI support
Constipation prevention
Senna
⸻
3. Antibiotic Strategy
Primary Prophylaxis
Typical regimen:
Cefazolin 2–3 g IV
Admin within 60 min of incision
Alternatives:
Vancomycin
Clindamycin
Considerations:
MRSA history
BMI
Revision TKA
Allergy profile
⸻
Antibiotic-Loaded Cement (Selected Cases)
Potential agents:
Gentamicin
Tobramycin
Vancomycin
Higher utilization:
Revision arthroplasty
Infection risk patients
⸻
4. Blood Management Layer
Tranexamic Acid (TXA)
Common delivery:
IV TXA
Topical TXA
Combined
Clinical goals:
Reduced EBL
Lower transfusion rate
Less hemarthrosis
Typical protocols:
1 g IV pre-incision
Repeat dose closure/postop
⸻
5. Multimodal Analgesia Stack
Typical ERAS pathway:
Preoperative
Celecoxib
Acetaminophen
Gabapentinoid
Intraoperative
Regional block
Periarticular injection
Postoperative
NSAID
Scheduled APAP
Opioid rescue
⸻
Periarticular Injection Cocktail
Institution-specific.
Potential components:
Ropivacaine
Epinephrine
Ketorolac
Morphine
Steroid
Goals:
Reduced early pain
Lower narcotic exposure
Improved ROM
⸻
6. Regional Anesthesia Intelligence
Current trend:
Adductor Canal Block
Advantages:
Quadriceps preservation
Early ambulation
Lower fall risk
Additional options:
Femoral block
IPACK
Genicular techniques
⸻
7. Anticoagulation Strategy
Risk-stratified protocols increasingly common.
Risk Profile
Common Approach
Standard Risk
Aspirin
Elevated Risk
LMWH
High Risk
DOAC / tailored therapy
Variables:
Prior VTE
BMI
Cancer
Hypercoagulable state
Revision surgery
⸻
8. Emerging Pharma Intelligence
Future-facing TKA pharmacology includes:
Long-Acting Local Anesthetics
Examples:
Liposomal bupivacaine
⸻
Personalized Analgesia
Potential AI-guided strategies:
Opioid responsiveness
Genetic metabolism profiles
Risk prediction
⸻
Infection Prevention Expansion
Research areas:
Local antimicrobials
Implant coatings
Precision prophylaxis
⸻
LDS Professional Intelligence Layer
TKA pharmaceutical management is becoming a precision system—not simply medication administration.
The future model is:
Procedure + Implant + Pharma + Data + Personalized Recovery
This pharma layer supports the LDS vision of a Procedure Builder, where medications, anesthesia, implants, and recovery pathways become transparent, customizable, and intelligence-driven.
-
Total Knee Digital Module, Section 10: Risks and complications
Total Knee Digital Module
Section 10: Risks and Complications
Patient-Facing Version
Understanding the Risks of Total Knee Replacement
A Total Knee Replacement (TKR) is one of the most successful orthopedic procedures performed today, helping patients reduce pain, improve mobility, and return to daily activities. While most procedures are completed safely with excellent outcomes, every surgery carries potential risks and complications.
Let’s Do Surgery believes informed patients make better decisions.
Understanding possible complications helps patients recognize warning signs and participate in safer recovery.⸻
Common Surgical Risks
1. Infection
Infection may occur at the incision site or deeper around the knee implant.
What Patients Should Watch For
Redness
Warmth around incision
Drainage
Fever
Increasing pain
Swelling
Treatment May Include
Antibiotics
Wound care
Surgical cleaning (irrigation and debridement)
Rarely, implant removal or revision surgery
LDS Visual Layer
“Inside an Infection” 3D animation showing bacteria around an implant and immune response.
⸻
2. Blood Clots (Deep Vein Thrombosis – DVT)
After surgery, decreased movement may allow blood clots to form in the leg veins.
Symptoms
Calf pain
Swelling
Tenderness
Warmth
Leg discoloration
If a clot travels to the lungs (Pulmonary Embolism – PE), it becomes a medical emergency.
Emergency Symptoms
Chest pain
Shortness of breath
Rapid heartbeat
Sudden dizziness
Prevention
Early walking
Compression devices
Blood-thinning medications
Leg exercises
LDS Animation
“How Blood Clots Form After Surgery.”
⸻
3. Bleeding and Hematoma
Some bleeding is expected after surgery, but excessive bleeding or blood collection (hematoma) may require treatment.
Possible Signs
Rapid swelling
Bruising
Increasing pain
Wound drainage
Treatment
Observation
Compression
Rarely return to operating room
⸻
4. Implant Loosening or Failure
Artificial knee components may loosen or wear over time.
Causes
Implant wear
Bone loss
High activity
Infection
Mechanical stress
Symptoms
New pain
Instability
Clicking
Reduced function
Possible Treatment
Physical therapy
Revision surgery
⸻
5. Knee Stiffness and Limited Motion
Some patients develop reduced flexibility following surgery.
Risk Factors
Scar tissue
Delayed rehabilitation
Severe preoperative stiffness
Pain limiting motion
Management
Aggressive physical therapy
Home exercises
Manipulation under anesthesia (MUA) if needed
Recovery Goal
Most patients aim for:
90° flexion for daily activities
110–120° for greater comfort and mobility
⸻
6. Persistent Pain
Most patients experience major pain improvement, but some continue to have discomfort.
Causes May Include
Scar sensitivity
Nerve irritation
Implant alignment issues
Infection
Soft tissue imbalance
LDS Patient Education
Pain Mapping Tool showing common pain locations and potential causes.
⸻
7. Nerve or Blood Vessel Injury
Important nerves and blood vessels travel behind the knee.
Although uncommon, injury may occur.
Symptoms
Numbness
Tingling
Weakness
Foot drop
Circulation changes
Management
Observation
Neurologic evaluation
Rare surgical repair
⸻
8. Instability or Dislocation
The knee may feel unstable if ligament balance or implant positioning is imperfect.
Symptoms
Buckling
Giving way
Feeling loose
Difficulty walking
Treatment
Bracing
Therapy
Revision surgery if severe
⸻
9. Fracture Around the Implant (Periprosthetic Fracture)
Bone surrounding the implant may fracture during or after surgery.
Higher Risk Patients
Osteoporosis
Falls
Older adults
Revision surgery
Treatment
Plates
Screws
Revision implants
⸻
10. Allergic or Material Sensitivity
Rarely, patients may react to implant materials.
Possible Symptoms
Persistent swelling
Skin irritation
Pain
Implant Materials May Include
Cobalt-chrome
Titanium
Polyethylene
Ceramic options
Preoperative allergy discussion may be helpful.
⸻
11. Anesthesia Risks
Anesthesia is generally very safe but carries potential risks.
Possible Complications
Nausea
Vomiting
Temporary confusion
Allergic reactions
Breathing issues
Cardiac complications
The anesthesia team evaluates these risks before surgery.
⸻
12. Revision Surgery
Some knee replacements eventually require another operation.
Reasons
Implant wear
Infection
Loosening
Fracture
Instability
Revision surgery is typically more complex than first-time replacement.
⸻
Warning Signs — When to Call Your Surgeon
Patients should seek medical attention for:
✓ Fever
✓ Increasing redness
✓ Drainage
✓ Severe swelling
✓ Calf pain
✓ Shortness of breath
✓ Chest pain
✓ Sudden inability to move the knee
✓ Worsening pain⸻
Professional-Facing Version
Risk and Complication Intelligence Layer
Total Knee Arthroplasty complications involve mechanical, infectious, thromboembolic, neurovascular, and biologic domains. Prevention depends on patient optimization, operative precision, and coordinated postoperative care.
⸻
Major Complication Categories
Category
Examples
Prevention Strategy
Infectious
Superficial/deep PJI
Antibiotics, sterile technique, optimization
Thromboembolic
DVT / PE
Chemoprophylaxis, early mobilization
Mechanical
Loosening, instability
Alignment and ligament balancing
Neurovascular
Nerve/vessel injury
Exposure awareness
Motion-related
Arthrofibrosis
Early ROM protocol
Biologic
Metal sensitivity
Patient selection
⸻
Periprosthetic Joint Infection (PJI)
Risk Factors
Diabetes
Obesity
Smoking
Malnutrition
Immunosuppression
Prior surgery
Diagnostic Workup
ESR
CRP
Synovial aspiration
Cell count
Culture
Imaging
Treatment Pathways
DAIR
One-stage revision
Two-stage revision
⸻
Arthrofibrosis
Contributors
Delayed rehab
Pain inhibition
Poor pre-op ROM
Technical factors
Intervention
Intensive PT
MUA
Arthroscopic lysis
Revision if structural cause exists
⸻
Mechanical Failure
Failure Modes
Aseptic loosening
Polyethylene wear
Malalignment
Instability
Patellofemoral dysfunction
Professional LDS Overlay
Alignment and balancing simulator comparing mechanical and kinematic alignment effects.
⸻
Neurovascular Considerations
Structures at Risk
Common peroneal nerve
Popliteal artery
Genicular vessels
High-Risk Situations
Severe deformity
Revision surgery
Posterior capsular release
Flexion contracture correction
⸻
Implant Survivorship and Revision Intelligence
Typical implant survival:
Time
Estimated Survivorship
10 years
90–95%
15 years
85–90%
20 years
Variable
Revision burden influenced by:
Implant design
Surgical technique
Activity level
Patient biology
Infection prevention
⸻
LDS Intelligence Layer
Risks Are Not Just Problems — They Are Decision Points
The LDS Total Knee Module frames complications as part of Decision → Direction → Connection:
Decision
Understand realistic risks
Compare implant and approach options
Review complication probabilities
Direction
Match with appropriate surgeon and center
Identify high-volume arthroplasty programs
Technology and revision capability overlays
Connection
Surgeon
Physical therapy
Implant manufacturers
Pharma and rehabilitation support
⸻
LDS Visual + Digital Assets
Patient Layer
3D complication library
Blood clot animation
Infection simulator
Recovery warning dashboard
Voice-guided complication education
Professional Layer
Revision intelligence dashboard
Failure mode analytics
Implant survivorship tracking
Risk prediction modeling
Registry integration concepts
LDS Principle:
“The safest surgery is informed, optimized, and connected.” -
Total Knee Digital Module, Section 11: Recovery pathway
Total Knee Digital Module
Section 11: Recovery Pathway
LDS Format | Patient-Facing + Professional Intelligence Layer
Theme: Communication as the Lifeline of Care⸻
SECTION 11 — RECOVERY PATHWAY
Patient-Facing Version
Recovery After Total Knee Replacement (TKA)
What Happens After Surgery?
A Total Knee Replacement (TKA) recovery is a step-by-step healing process designed to:
Reduce pain
Restore movement
Improve walking and function
Build strength and stability
Return patients to everyday life
Recovery begins immediately after surgery and continues for several months.
The most important part of recovery is:
Movement + Rehabilitation + Communication with your care team.
⸻
Phase 1: Immediate Recovery (0–24 Hours)
Recovery Room (PACU)
After surgery, patients are moved to the:
Post-Anesthesia Care Unit (PACU)
The care team monitors:
Blood pressure
Heart rate
Oxygen level
Pain control
Nausea
Leg circulation
Surgical dressing
Common experiences:
Grogginess
Knee numbness
Swelling
Tightness
Mild discomfort
Many patients receive:
Ice therapy
Compression devices
Pain medication
Early mobilization support
⸻
Early Walking
Most patients stand and walk:
Within hours of surgery
A physical therapist assists with:
Standing
Weight-bearing
Walker use
Short hallway walking
This helps prevent:
Blood clots
Lung complications
Muscle weakness
Joint stiffness
⸻
Phase 2: Hospital or Surgery Center Recovery (Day 1–3)
Modern knee replacement recovery is often:
Same-day discharge
Overnight stay
Short inpatient stay
Depends on:
Age
Medical history
Home support
Pain control
Mobility
Goals before discharge:
✓ Safe walking
✓ Controlled pain
✓ Knee bending progress
✓ Bathroom independence
✓ Understanding home instructions⸻
Pain Management During Recovery
Pain is expected but usually manageable.
Pain control uses a multimodal approach:
Nerve blocks
Local anesthetic
Acetaminophen
NSAIDs
Limited opioids
Ice and elevation
Physical therapy
Patients often describe pain as:
Pressure
Tightness
Muscle soreness
Swelling discomfort
Severe uncontrolled pain should be reported.
⸻
Phase 3: Home Recovery (Week 1–6)
This is the most active recovery phase.
Daily goals include:
Walking more
Improving motion
Reducing swelling
Regaining strength
Increasing independence
Common tools:
Walker
Cane
Compression stockings
Ice machine
Exercise program
⸻
Typical Motion Milestones
Common rehabilitation goals:
Week 1–2:
Knee straightening
70–90° flexion
Week 3–6:
90–120° flexion
Improved walking
Stair training
Flexibility improves gradually.
Every patient heals differently.
⸻
Physical Therapy
Physical therapy is one of the most important parts of recovery.
Goals:
Restore motion
Improve balance
Build strength
Normalize walking
Typical exercises:
Heel slides
Quad sets
Straight leg raises
Stationary bike
Gait training
Therapy may occur:
Home PT
Outpatient PT
Hybrid programs
Digital rehabilitation platforms
⸻
Managing Swelling
Swelling is normal.
It may last:
Weeks
Sometimes months
Helpful strategies:
Ice
Leg elevation
Compression
Walking
Avoiding prolonged sitting
Swelling usually improves gradually.
⸻
Phase 4: Functional Recovery (6–12 Weeks)
Most patients notice:
Less pain
Better walking
Improved stability
Greater confidence
Common milestones:
Driving (provider dependent)
Returning to desk work
Improved sleep
Reduced assistive device use
Many patients resume:
Shopping
Social activities
Light exercise
⸻
Phase 5: Long-Term Recovery (3–12 Months)
Healing continues long after surgery.
The knee becomes:
Stronger
Less swollen
More flexible
More natural feeling
Patients may continue improving for:
Up to one year
Goals include:
Comfortable walking
Improved endurance
Better quality of life
Long-term implant success
⸻
Warning Signs — When to Contact Your Surgeon
Call your care team if you develop:
Fever
Increasing redness
Drainage
Severe swelling
Chest pain
Shortness of breath
Calf pain
Sudden loss of motion
Uncontrolled pain
These may signal:
Infection
Blood clot
Implant complication
Medical emergency
⸻
LDS Recovery Timeline
Time
Typical Recovery Milestone
Day 0
Surgery + standing/walking
Day 1–3
Discharge + home transition
Week 1–2
Swelling control + motion gains
Week 3–6
Strength + walking improvement
Week 6–12
Functional recovery
Month 3–12
Continued healing + full adaptation
⸻
Professional-Facing Version
TKA Recovery Intelligence Layer
Recovery success depends on:
1. Enhanced Recovery Pathways (ERAS)
Protocols emphasize:
Early ambulation
Multimodal analgesia
Reduced opioid exposure
Shortened LOS
Patient education
⸻
2. Rehabilitation Metrics
Common monitored parameters:
ROM goals:
Full extension
90° flexion early
110–120° functional flexion
Functional scores:
KOOS
WOMAC
PROMIS
Oxford Knee Score
Mobility measures:
Timed Up and Go (TUG)
Gait assessment
Stair function
⸻
3. DVT Prevention
Standard strategies:
Mechanical:
SCDs
Early ambulation
Compression
Pharmacologic:
Aspirin
LMWH
DOACs
Institution-specific prophylaxis
Risk stratification is critical.
⸻
4. Postoperative Monitoring
Clinical surveillance includes:
Wound healing
Hematoma
Persistent drainage
Infection markers
Neurovascular status
Arthrofibrosis risk
Implant stability
⸻
5. Recovery Technologies
Emerging tools:
Remote monitoring
Wearable motion sensors
Digital PT platforms
Tele-rehabilitation
AI recovery analytics
Patient engagement apps
These technologies align with the LDS Direction + Connection model by extending care beyond the hospital.
⸻
LDS Patient Decision Support
Patients commonly ask:
How long until I walk normally?
How much pain should I expect?
When can I drive?
Will therapy hurt?
How long before my new knee feels natural?
LDS Recovery Principle:
Recovery is not just healing from surgery — it is learning how to move, function, and live with a new joint.
-
Total Knee Digital Module,
Section 12: Patient decision support
Total Knee Digital Module
Section 12: Patient Decision Support
Patient-facing version
Should I consider total knee replacement?
Total knee replacement may be considered when knee arthritis or joint damage is severely affecting daily life and non-surgical treatments are no longer working.
You may be ready to discuss surgery if you have:
Knee pain that limits walking, stairs, standing, sleep, or daily activities
Pain that continues despite medications, injections, bracing, weight loss, or physical therapy
Stiffness, swelling, instability, or deformity of the knee
X-rays showing advanced arthritis or joint space loss
A major decline in quality of life
The goal of total knee replacement is not just to replace the joint. The goal is to help the patient return to safer movement, less pain, and better function.
⸻
The patient decision pathway
1. Understand the problem
The patient should know:
What is wrong with my knee?
Most total knee replacements are done for severe osteoarthritis, but they may also be needed for rheumatoid arthritis, post-traumatic arthritis, deformity, or failed prior surgery.Is the whole knee affected or only one compartment?
This helps determine whether the patient may need total knee replacement or a partial knee replacement.How bad is the arthritis?
X-rays, exam findings, pain level, and functional limitations all help guide the decision.⸻
2. Understand the options
Before surgery, patients should understand the full treatment ladder:
Non-surgical options
Activity modification
Physical therapy
Anti-inflammatory medications
Weight loss when appropriate
Bracing
Corticosteroid injections
Viscosupplementation in select cases
Assistive devices such as a cane
Surgical options
Total knee replacement
Partial knee replacement
Revision knee replacement if a prior implant has failed
Realignment procedures in select younger patients
The best option depends on the patient’s anatomy, arthritis pattern, age, activity goals, health status, and expectations.
⸻
3. Understand the procedure
A total knee replacement removes damaged cartilage and bone from the ends of the femur and tibia and replaces them with metal and plastic implant components.
The patient should understand:
What parts of the knee are replaced
Whether the kneecap may be resurfaced
What type of implant may be used
Whether the procedure will use manual instruments, navigation, robotics, or patient-specific planning
What anesthesia options are available
What pain-control plan will be used
What recovery will look like after surgery
⸻
Key patient questions
Diagnosis questions
Do I have osteoarthritis, rheumatoid arthritis, or another knee problem?
Is my arthritis mild, moderate, or severe?
Is the arthritis in one compartment or the entire knee?
Do my symptoms match my X-rays?
Are there other sources of pain, such as hip or spine problems?
Treatment questions
Have I tried enough non-surgical treatment?
Would more therapy, injections, weight loss, or bracing help?
Am I a candidate for partial knee replacement?
Why are you recommending total knee replacement instead of another option?
What happens if I wait?
Surgeon questions
How many total knee replacements do you perform each year?
Do you perform robotic-assisted or computer-navigated knee replacement?
What implant systems do you commonly use?
What is your infection rate, readmission rate, and revision rate?
Where will the surgery be performed?
Hospital or surgery center questions
Is this done inpatient or outpatient?
Does the facility perform a high volume of knee replacements?
What emergency support is available?
Will I go home the same day or stay overnight?
What physical therapy support is available after surgery?
Implant and technology questions
What implant brand or design will be used?
Is the implant cemented or cementless?
Will robotics or navigation be used?
How does the technology improve alignment, planning, or soft-tissue balancing?
Are there added costs or insurance considerations?
Recovery questions
How much pain should I expect?
When will I walk?
When can I climb stairs?
When can I drive?
When can I return to work?
How long will I need physical therapy?
What range of motion should I expect?
What activities should I avoid after surgery?
⸻
Patient decision scorecard
Patients can use this simple scorecard to organize the decision.
Decision Factor
Low Concern
Moderate Concern
High Concern
Daily knee pain
☐
☐
☐
Trouble walking
☐
☐
☐
Difficulty with stairs
☐
☐
☐
Sleep disruption
☐
☐
☐
Loss of independence
☐
☐
☐
Failed non-surgical care
☐
☐
☐
X-ray arthritis severity
☐
☐
☐
Fear of surgery
☐
☐
☐
Recovery support at home
☐
☐
☐
Work or caregiver responsibilities
☐
☐
☐
Decision guide:
If pain, function loss, and failed non-surgical care are high, the patient may be ready for a surgical consultation. If fear, medical risk, or lack of home support are high, the patient may need more preparation before surgery.⸻
Shared decision-making model
The best decision is made when the patient, surgeon, care team, and support system understand the same plan.
Patient priorities
The patient may care most about:
Pain relief
Walking farther
Climbing stairs
Returning to work
Avoiding a nursing facility
Staying independent
Returning to golf, biking, swimming, or travel
Avoiding complications
Understanding implant and technology choices
Surgeon priorities
The surgeon evaluates:
Arthritis severity
Knee alignment and deformity
Range of motion
Ligament stability
Bone quality
Medical risk
Infection risk
Realistic outcome expectations
Implant and technique selection
Care team priorities
The care team helps coordinate:
Medical clearance
Pre-op education
Pain management
Physical therapy
Home safety
Discharge planning
Follow-up appointments
⸻
“Am I ready?” checklist
A patient may be ready for total knee replacement when:
☐ I understand my diagnosis
☐ I understand non-surgical and surgical options
☐ My pain or disability affects my quality of life
☐ I have tried reasonable non-surgical care
☐ I understand the risks and benefits
☐ I understand the recovery timeline
☐ I have a support plan for the first 1–2 weeks
☐ I understand that physical therapy is critical
☐ I have realistic expectations
☐ I have chosen a surgeon and facility I trust
⸻
Professional-facing version
Decision-support objective
The patient decision support layer helps convert diagnosis, imaging, symptoms, comorbidities, goals, and available technology into a structured total knee arthroplasty decision pathway.
The purpose is to support:
Appropriateness of surgery
Patient education
Expectation alignment
Surgeon selection
Facility selection
Implant and technology transparency
Recovery planning
Risk reduction
⸻
Clinical decision framework
1. Indication assessment
Total knee arthroplasty is generally considered when there is:
Advanced symptomatic knee arthritis
Persistent pain despite appropriate conservative management
Functional limitation affecting activities of daily living
Radiographic joint degeneration
Failure of non-operative treatment
Patient willingness to participate in rehabilitation
Common indications include:
Primary osteoarthritis
Rheumatoid arthritis
Post-traumatic arthritis
Severe varus or valgus deformity
Failed osteotomy or prior knee surgery
Avascular necrosis involving the knee in select cases
⸻
2. Contraindication and optimization screen
Before proceeding, evaluate:
Active infection
Poorly controlled diabetes
Severe vascular disease
Severe cardiopulmonary risk
Open wounds or skin breakdown
Severe obesity-related risk
Active dental or systemic infection concerns
Poor home support
Unrealistic expectations
Inability or unwillingness to participate in rehab
Optimization may include:
Hemoglobin A1c management
Smoking cessation
Weight reduction when appropriate
Dental or infection clearance
Cardiac clearance
Medication review
Anticoagulation planning
Nutrition assessment
Prehabilitation
⸻
LDS Patient Decision Engine
Input layer
The platform should collect:
Input Category
Data Points
Symptoms
Pain level, duration, stiffness, swelling, instability
Function
Walking distance, stairs, work limits, sleep disruption
Imaging
X-ray severity, compartment involvement, deformity
Prior treatment
PT, injections, medications, bracing, weight loss
Medical risk
Diabetes, BMI, smoking, cardiac history, anticoagulation
Patient goals
Pain relief, work, sports, travel, independence
Support system
Home assistance, transportation, PT access
Technology preference
Robotics, navigation, implant transparency
Location
ZIP code, travel radius, preferred facility type
⸻
Output layer
The decision engine should generate:
1. Surgery readiness status
Not ready yet
Patient may benefit from further non-operative care, optimization, imaging, or second opinion.Possibly ready
Patient has significant symptoms but needs more evaluation, education, or medical preparation.Likely ready for surgical consult
Patient has advanced symptoms, failed conservative treatment, imaging correlation, and realistic goals.⸻
2. Recommended next step
Examples:
Schedule orthopedic evaluation
Obtain standing weight-bearing knee X-rays
Try structured physical therapy
Discuss injection options
Begin medical optimization
Consider partial vs total knee replacement evaluation
Seek second opinion
Review robotic-assisted TKA options
Build home recovery plan
⸻
3. Patient education match
The system should display targeted education modules based on patient needs:
Severe pain but mild imaging → “Why symptoms and imaging may not match”
Severe arthritis, high fear → “What happens step-by-step during surgery”
High BMI or diabetes → “How optimization lowers complication risk”
Lives alone → “Planning home support after knee replacement”
Tech interest → “Robotic vs manual knee replacement”
Younger patient → “Implant longevity and revision risk”
Work concern → “Return-to-work planning”
⸻
Surgeon matching criteria
The LDS platform can match patients based on:
Matching Factor
Patient Need
High-volume TKA surgeon
Standard primary TKA
Robotic-assisted TKA surgeon
Technology-focused patient
Revision specialist
Failed prior implant or complex history
Complex deformity surgeon
Severe varus, valgus, flexion contracture
Outpatient-capable surgeon
Healthy patient seeking same-day discharge
Hospital-based surgeon
Higher medical-risk patient
Partial knee specialist
Isolated compartment arthritis
Rapid-recovery program
Patient prioritizing faster mobility
⸻
Facility matching criteria
Facility decision support should consider:
Inpatient hospital vs ambulatory surgery center
Joint replacement volume
Infection-prevention protocols
Anesthesia and regional block capability
Physical therapy access
Emergency backup
ICU availability for higher-risk patients
Robotic or navigation platform availability
Same-day discharge program
Bundled payment or insurance network status
⸻
Patient decision-support UI concept
Screen 1: “Tell us about your knee”
Inputs:
Which knee hurts?
Pain score
Walking distance
Stairs difficulty
Night pain
Swelling
Instability
Prior treatments
Screen 2: “What have you tried?”
Inputs:
Physical therapy
NSAIDs or pain medication
Cortisone injection
Gel injection
Weight loss
Brace
Cane/walker
Prior surgery
Screen 3: “What do your images show?”
Inputs:
Mild, moderate, or severe arthritis
Bone-on-bone arthritis
Varus or valgus alignment
One-compartment vs multi-compartment disease
Upload X-ray option
Screen 4: “What matters most to you?”
Inputs:
Pain relief
Walking
Stairs
Work
Sports
Travel
Independence
Fast recovery
Technology options
Avoiding hospital stay
Screen 5: “Your decision pathway”
Outputs:
Readiness category
Recommended next step
Questions to ask surgeon
Surgeon/facility match type
Recovery preparation checklist
⸻
LDS conversion layer
The Patient Decision Support section should drive the user toward action:
Primary CTA
Build My Knee Replacement Plan
Secondary CTAs
Compare Surgeons Near Me
Explore Robotic Knee Replacement
Download My Surgery Readiness Checklist
Ask for a Second Opinion
See What Happens Step-by-Step⸻
Patient-facing closing statement
Total knee replacement is a major decision. The right choice depends on your pain, your X-rays, your daily function, your health, your goals, and your support system.
Let’s Do Surgery helps patients understand the decision before they enter the operating room — so they can ask better questions, compare options, and choose the path that fits them best.
-
Total Knee Digital Module,
Section 13: Professional intelligence layer
Total Knee Digital Module
Section 13: Professional Intelligence Layer
Purpose
The Professional Intelligence Layer turns the Total Knee Replacement module from patient education into a clinical, operational, and industry-facing intelligence system.
It helps surgeons, hospitals, reps, device companies, and care teams understand:
How the procedure is built, why certain choices are made, what products are used, and how outcomes can be improved.
⸻
1. Professional-Facing Overview
Total Knee Replacement is not just one procedure.
It is a customizable reconstruction of the knee joint based on:
Patient anatomy
Severity of arthritis or deformity
Ligament stability
Bone quality
Implant philosophy
Surgeon preference
Robotic/navigation availability
Hospital supply contracts
Recovery goals
The professional layer explains how each decision affects the final surgical plan.
⸻
2. Core Professional Questions
This section should answer:
What implant design is best for this patient?
Should the case be manual, navigated, or robotic-assisted?
Should the posterior cruciate ligament be retained or substituted?
Is the deformity varus, valgus, flexion contracture, or complex?
What fixation strategy is best: cemented, cementless, or hybrid?
What bearing surface and polyethylene insert are appropriate?
What intraoperative tools, trials, saw guides, cement, implants, and pharma products are needed?
⸻
3. Professional Decision Engine
A. Patient Factors
Inputs:
Age
BMI
Activity level
Bone quality
Diabetes status
Smoking status
Prior surgery
Prior infection
Inflammatory arthritis
Severe deformity
Revision risk
Home support
Output:
Risk-adjusted surgical pathway.
⸻
B. Anatomy & Deformity Factors
Inputs:
Varus knee
Valgus knee
Flexion contracture
Bone loss
Patellar tracking
Ligament balance
Rotational alignment
Tibial slope
Femoral/tibial sizing
Soft tissue envelope
Output:
Implant, alignment, and balancing strategy.
⸻
C. Technology Factors
Inputs:
Manual instrumentation
Computer navigation
Patient-specific instruments
Robotic-assisted TKA
CT-based planning
Imageless robotic platforms
Intraoperative balancing tools
Output:
Procedure technology recommendation.
⸻
4. Implant Intelligence Layer
Implant Categories
Category
Professional Consideration
Cruciate-retaining
Preserves PCL when stable and functional
Posterior-stabilized
Uses cam-post mechanism when PCL is removed or deficient
Medial-pivot
Designed to recreate medial stability and kinematics
Constrained condylar
Used for instability, deformity, or ligament insufficiency
Hinged knee
Used for severe instability, major bone loss, tumor, or complex revision
Cementless implants
Often considered in younger or good bone-quality patients
Cemented implants
Common standard for reliable fixation
⸻
5. Device & Supply Intelligence
Core Device Stack
Femoral component
Tibial baseplate
Polyethylene insert
Patellar component
Trial implants
Alignment guides
Cutting blocks
Saw blades
Tibial/femoral preparation instruments
Cement restrictors if needed
Bone cement
Pulse lavage
Tourniquet
Suction/drain supplies
Closure materials
Dressings
Advanced Technology Stack
Robotic planning workstation
CT or imageless planning system
Tracking pins/arrays
Robotic arm or navigation camera
Ligament balancing software
Gap assessment tools
Smart trialing systems
⸻
6. Pharma Intelligence Layer
Pre-op
Antibiotic prophylaxis
Tranexamic acid protocol
VTE risk stratification
Regional anesthesia plan
Diabetes optimization
MRSA/MSSA screening/decolonization
Intra-op
IV antibiotics
IV/topical TXA
Local infiltration analgesia
Periarticular injection cocktail
Cement additives when indicated
Antiseptic irrigation protocols
Post-op
Multimodal pain control
NSAID or COX-2 inhibitor when appropriate
Acetaminophen
Short-course opioid rescue
Anticoagulation or aspirin pathway
Antiemetics
Bowel regimen
Infection surveillance
⸻
7. OR Workflow Intelligence
Professional Workflow Map
Patient selection
Imaging and templating
Implant planning
Anesthesia and block
Positioning and prep
Exposure
Femoral and tibial bone preparation
Gap balancing
Trialing
Patellar assessment/resurfacing decision
Final component implantation
Cementation or press-fit fixation
Closure
Dressing
Recovery and mobilization
⸻
8. Risk Intelligence Dashboard
Key Risks to Track
Periprosthetic joint infection
DVT/PE
Stiffness
Arthrofibrosis
Instability
Malalignment
Patellar maltracking
Aseptic loosening
Polyethylene wear
Periprosthetic fracture
Wound complications
Revision surgery
Risk Scoring Outputs
Low-risk outpatient pathway
Standard inpatient pathway
High-risk optimization pathway
Complex deformity pathway
Revision-risk pathway
⸻
9. Rep & Industry Intelligence
Rep-Facing Value
This module helps reps understand:
Which implant systems are used
Which surgeons use robotic platforms
Which hospitals perform high-volume TKA
Which products are needed for each case type
Which cases require advanced constraint or revision options
Where implant conversion opportunities exist
Industry Data Fields
Implant manufacturer
Implant family
Cemented vs cementless usage
Robotic vs manual case
Polyethylene type
Patella resurfaced or not
Case complexity
Length of stay
Discharge destination
Complications
Revision risk
Surgeon volume tier
Hospital technology profile
⸻
10. Professional Builder Logic
“Build This Total Knee”
Professional users can configure:
Approach
Medial parapatellar
Subvastus
Midvastus
Quadriceps-sparing
Alignment Philosophy
Mechanical alignment
Kinematic alignment
Functional alignment
Restricted kinematic alignment
Technology
Manual
Navigation
PSI
Robotic-assisted
Implant Design
CR
PS
Medial-pivot
Constrained
Hinged
Fixation
Cemented
Cementless
Hybrid
Patella Strategy
Resurface
Do not resurface
Selective resurfacing
Recovery Pathway
Same-day discharge
23-hour observation
Inpatient admission
Rehab facility pathway
⸻
11. Surgeon Intelligence Layer
Surgeon Profile Data
TKA annual volume
Revision experience
Robotic platform experience
Preferred implant system
Hospital affiliations
Outpatient TKA capability
Complex deformity experience
Infection/revision management
Patient-reported outcomes
Telehealth availability
Surgeon Matching Labels
High-Volume Total Knee Surgeon
Robotic Knee Replacement Specialist
Complex Deformity Specialist
Outpatient Joint Replacement Surgeon
Revision Knee Specialist
Cementless Implant Specialist
Same-Day Discharge Specialist
⸻
12. Hospital Intelligence Layer
Hospital Profile Data
Annual TKA volume
Robotic platform availability
Navigation capability
Infection prevention program
Joint replacement certification
ASC vs hospital setting
ICU availability
Rehab partnerships
Bundled payment participation
Readmission rates
Discharge-to-home rates
Hospital Matching Labels
Closest Joint Replacement Center
High-Volume Orthopedic Hospital
Robotic Joint Replacement Center
Outpatient Surgery Center Option
Complex Case Hospital
Revision-Capable Facility
⸻
13. AI Professional Assistant
Use Cases
The AI assistant can help professionals:
Compare implant options
Build a case plan
Identify missing supplies
Create a preference card
Map pharma needs
Explain robotic vs manual workflow
Flag risk factors
Prepare rep questions
Generate patient-facing explanations
Build post-op recovery instructions
Example Prompt
“Build a professional TKA plan for a 68-year-old active patient with varus osteoarthritis, good bone quality, BMI 31, and interest in same-day discharge.”
Example Output
Candidate for primary TKA
Consider CR or medial-pivot implant if PCL appropriate
Cemented or cementless depending on bone quality and surgeon preference
Robotic-assisted planning may improve alignment precision
TXA protocol recommended if no contraindication
Aspirin-based VTE pathway may be considered if low risk
Same-day discharge possible if pain control, mobility, and home support are adequate
⸻
14. Data Architecture
Core Tables
Patient Factors Table
Age
BMI
Activity level
Comorbidities
Deformity type
Bone quality
Infection risk
VTE risk
Discharge readiness
Procedure Plan Table
Approach
Technology
Implant design
Fixation
Patella strategy
Alignment philosophy
Bearing type
Closure method
Device Table
Manufacturer
Implant family
Component type
SKU
Size range
Cement compatibility
Robotic compatibility
Pharma Table
Drug class
Medication
Timing
Dose range
Indication
Contraindications
Related pathway
Outcome Table
OR time
Length of stay
Pain score
Range of motion
Discharge destination
Complication
Readmission
Revision
⸻
15. LDS Monetization Layer
Revenue Opportunities
Sponsored implant education
Robotic platform placement
Rep lead generation
Surgeon profile upgrades
Hospital technology listings
Device marketplace referrals
Patient education licensing
Professional preference-card builder
Data dashboards for industry
Sponsored recovery pathway tools
Industry Dashboard Examples
TKA implant trend dashboard
Robotic adoption dashboard
Cemented vs cementless trend map
Surgeon volume and technology map
Hospital outpatient TKA readiness map
Product opportunity dashboard
⸻
16. Final LDS Positioning Statement
The Total Knee Professional Intelligence Layer transforms knee replacement from a static procedure description into a dynamic surgical planning, product selection, and care-navigation engine.
It connects:
Patient need → surgical decision → implant selection → device stack → pharma pathway → surgeon match → hospital capability → recovery outcome.
